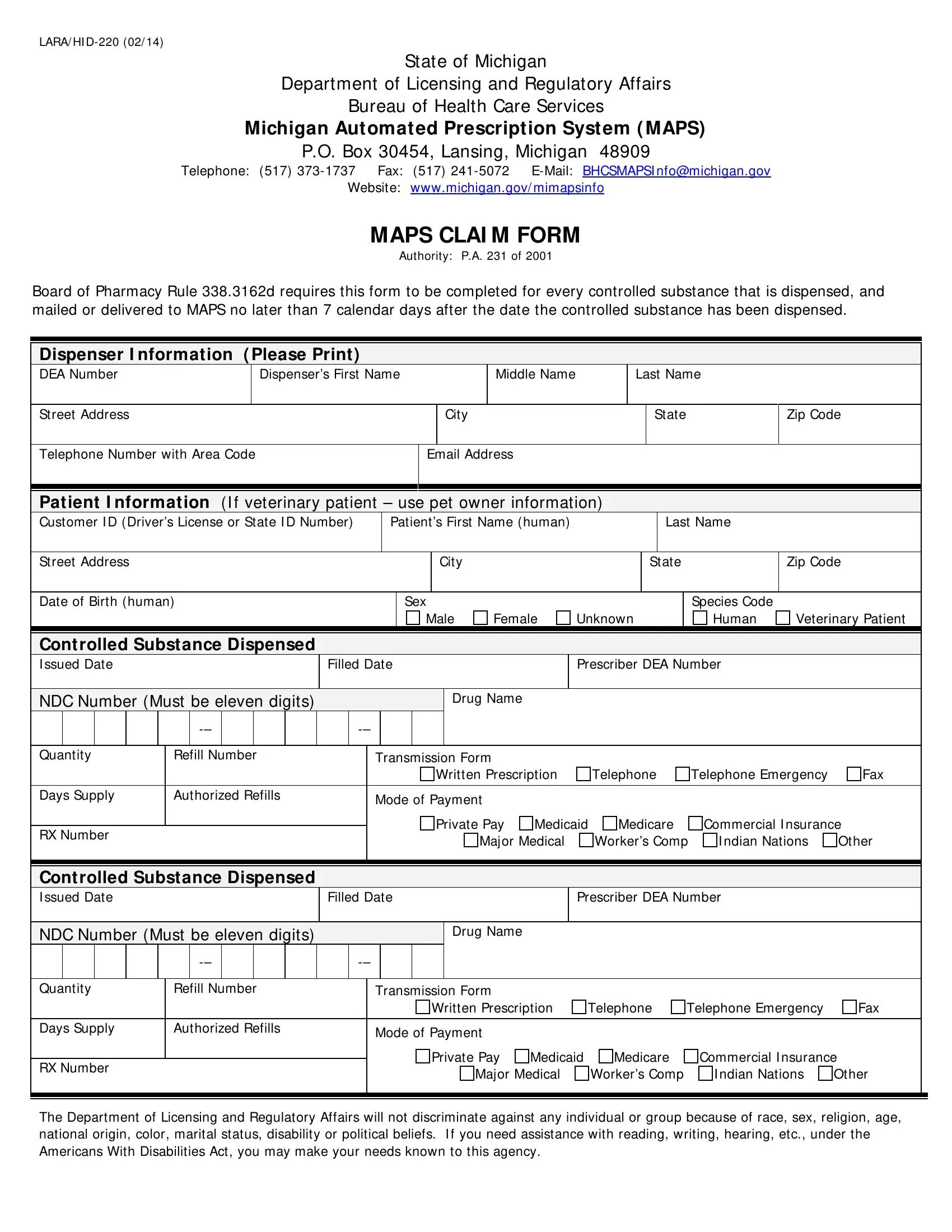
In an effort to regulate and monitor the dispensation of controlled substances, the State of Michigan’s Department of Licensing and Regulatory Affairs has implemented a critical tool: the LARA/HI D-220 form, under the purview of the Michigan Automated Prescription System (MAPS). This form plays a fundamental role in combating the misuse and abuse of prescription drugs, ensuring that every dispensed controlled substance is accounted for. It entails detailed sections for both dispenser and patient information, including the dispenser's DEA number, and for patients, involves a thorough capture of personal details and the specifics of the controlled substance dispensed - from the drug name to the quantity and mode of payment. Noteworthy is the form's inclusiveness, accommodating information if the patient happens to be a veterinary one, hence enhancing its utility across a broader spectrum of the healthcare industry. The necessity for this form is underscored by Board of Pharmacy Rule 338.3162d, mandating its completion and submission within a stringent timeline post-dispensation, emphasizing the state’s commitment to diligent oversight and patient safety. Additionally, the directive encapsulates the state’s stance on non-discrimination and accessibility, ensuring equitable treatment and support for all individuals, including those with disabilities, underlining the form’s role not just as a regulatory requirement, but as a testament to ethical healthcare practices.
| Question | Answer |
|---|---|
| Form Name | Form Lara Hid 220 |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | cis_fhs_bhser_m apsclaimform4 09_316533_7 what is maps claim form in michigan |
LARA/ HI
State of Michigan
Department of Licensing and Regulatory Affairs
Bureau of Health Care Services
Michigan Aut omat ed Prescript ion Syst em ( MAPS)
P.O. Box 30454, Lansing, Michigan 48909
Telephone: (517)
Website: www.michigan.gov/ mimapsinfo
MAPS CLAI M FORM
Authority: P.A. 231 of 2001
Board of Pharmacy Rule 338.3162d requires this form to be completed for every controlled substance that is dispensed, and mailed or delivered to MAPS no later than 7 calendar days after the date the controlled substance has been dispensed.
Dispenser I nformat ion ( Please Print )
DEA Number |
|
Dispenser’s First Name |
|
|
Middle Name |
Last Name |
|
|
|
|
|
|
|
|
|
|
|
Street Address |
|
|
City |
|
State |
Zip Code |
||
|
|
|
|
|
|
|
||
Telephone Number with Area Code |
|
Email Address |
|
|
|
|||
|
|
|
|
|
|
|
|
|
Pat ient I nformat ion (I f veterinary patient – use pet owner information)
|
Customer I D (Driver’s License or State I D Number) |
|
|
Patient’s First Name (human) |
|
|
|
Last Name |
|
|
|
||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Street Address |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
City |
|
|
|
|
|
State |
|
|
Zip Code |
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Date of Birth (human) |
|
|
|
|
|
Sex |
|
|
|
|
|
|
|
|
|
Species Code |
|
|
|
|||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Male |
Female |
Unknown |
|
|
Human |
Veterinary Patient |
|
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Cont rolled Subst ance Dispensed |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||
|
I ssued Date |
|
|
|
|
|
|
Filled Date |
|
|
|
Prescriber DEA Number |
|
|
|
||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
NDC Number (Must be eleven digits) |
|
|
|
|
|
|
|
|
|
Drug Name |
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
Quantity |
|
Refill Number |
|
|
|
Transmission Form |
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Written Prescription |
|
Telephone |
|
Telephone Emergency |
Fax |
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
Days Supply |
|
Authorized Refills |
|
|
|
Mode of Payment |
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Private Pay |
Medicaid |
Medicare |
|
Commercial I nsurance |
|
|||||||||
|
RX Number |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Major Medical |
|
Worker’s Comp |
I ndian Nations |
Other |
|
||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Cont rolled Subst ance Dispensed |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||
|
I ssued Date |
|
|
|
|
|
|
Filled Date |
|
|
|
Prescriber DEA Number |
|
|
|
||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||
|
NDC Number (Must be eleven digits) |
|
|
|
|
|
|
|
|
|
Drug Name |
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
Quantity |
|
Refill Number |
|
|
|
Transmission Form |
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Written Prescription |
Telephone |
Telephone Emergency |
Fax |
|
|||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
Days Supply |
|
Authorized Refills |
|
|
|
Mode of Payment |
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Private Pay |
Medicaid |
Medicare |
|
Commercial I nsurance |
|
||||||||||
|
RX Number |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Major Medical |
|
Worker’s Comp |
|
I ndian Nations |
Other |
|
|||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
The Department of Licensing and Regulatory Affairs will not discriminate against any individual or group because of race, sex, religion, age, national origin, color, marital status, disability or political beliefs. I f you need assistance with reading, writing, hearing, etc., under the Americans With Disabilities Act, you may make your needs known to this agency.