In the world of business, there are certain universal truths that govern success. Among these is understanding one's target market and adapting products or services to meet their needs. Lara Hid 220 is a perfect example of a company that has done just this, creating an innovative product that meets the specific needs of its target market. In this post, we'll take a look at what makes Lara Hid 220 so unique and how it can benefit businesses both small and large. So without further ado, let's get started! What if there was a way for businesses to cut costs while simultaneously increasing efficiency? Enter Lara Hid 220- an innovative new product that allows businesses to save on printing expenses while still maintaining high quality print output. Created by Lara Corporation, this ground-breaking new system has quickly gained popularity among business owners nationwide due to its affordability and versatility. Here we'll take a closer look at what makes Lara Hid 220 so special and how
| Question | Answer |
|---|---|
| Form Name | Form Lara Hid 220 |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | cis_fhs_bhser_m apsclaimform4 09_316533_7 what is maps claim form in michigan |
LARA/ HI
State of Michigan
Department of Licensing and Regulatory Affairs
Bureau of Health Care Services
Michigan Aut omat ed Prescript ion Syst em ( MAPS)
P.O. Box 30454, Lansing, Michigan 48909
Telephone: (517)
Website: www.michigan.gov/ mimapsinfo
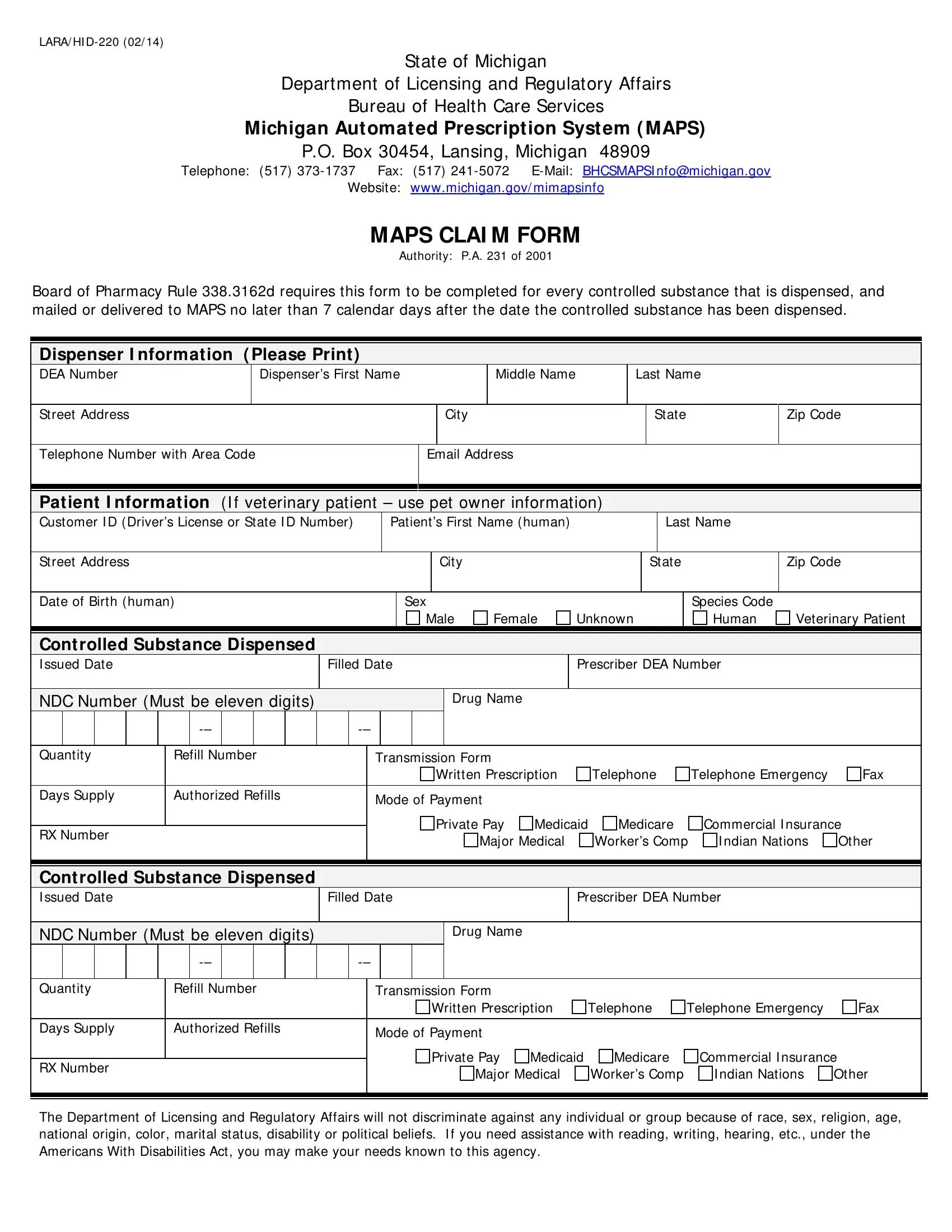
MAPS CLAI M FORM
Authority: P.A. 231 of 2001
Board of Pharmacy Rule 338.3162d requires this form to be completed for every controlled substance that is dispensed, and mailed or delivered to MAPS no later than 7 calendar days after the date the controlled substance has been dispensed.
Dispenser I nformat ion ( Please Print )
DEA Number |
|
Dispenser’s First Name |
|
|
Middle Name |
Last Name |
|
|
|
|
|
|
|
|
|
|
|
Street Address |
|
|
City |
|
State |
Zip Code |
||
|
|
|
|
|
|
|
||
Telephone Number with Area Code |
|
Email Address |
|
|
|
|||
|
|
|
|
|
|
|
|
|
Pat ient I nformat ion (I f veterinary patient – use pet owner information)
|
Customer I D (Driver’s License or State I D Number) |
|
|
Patient’s First Name (human) |
|
|
|
Last Name |
|
|
|
||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Street Address |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
City |
|
|
|
|
|
State |
|
|
Zip Code |
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Date of Birth (human) |
|
|
|
|
|
Sex |
|
|
|
|
|
|
|
|
|
Species Code |
|
|
|
|||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Male |
Female |
Unknown |
|
|
Human |
Veterinary Patient |
|
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Cont rolled Subst ance Dispensed |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||
|
I ssued Date |
|
|
|
|
|
|
Filled Date |
|
|
|
Prescriber DEA Number |
|
|
|
||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
NDC Number (Must be eleven digits) |
|
|
|
|
|
|
|
|
|
Drug Name |
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
Quantity |
|
Refill Number |
|
|
|
Transmission Form |
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Written Prescription |
|
Telephone |
|
Telephone Emergency |
Fax |
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
Days Supply |
|
Authorized Refills |
|
|
|
Mode of Payment |
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Private Pay |
Medicaid |
Medicare |
|
Commercial I nsurance |
|
|||||||||
|
RX Number |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Major Medical |
|
Worker’s Comp |
I ndian Nations |
Other |
|
||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Cont rolled Subst ance Dispensed |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||
|
I ssued Date |
|
|
|
|
|
|
Filled Date |
|
|
|
Prescriber DEA Number |
|
|
|
||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||
|
NDC Number (Must be eleven digits) |
|
|
|
|
|
|
|
|
|
Drug Name |
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
Quantity |
|
Refill Number |
|
|
|
Transmission Form |
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Written Prescription |
Telephone |
Telephone Emergency |
Fax |
|
|||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
Days Supply |
|
Authorized Refills |
|
|
|
Mode of Payment |
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Private Pay |
Medicaid |
Medicare |
|
Commercial I nsurance |
|
||||||||||
|
RX Number |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Major Medical |
|
Worker’s Comp |
|
I ndian Nations |
Other |
|
|||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
The Department of Licensing and Regulatory Affairs will not discriminate against any individual or group because of race, sex, religion, age, national origin, color, marital status, disability or political beliefs. I f you need assistance with reading, writing, hearing, etc., under the Americans With Disabilities Act, you may make your needs known to this agency.