Our PDF editor allows you to create documents. There's no need to do much to modify 2221a child abuse form documents. Just simply use these particular actions.
Step 1: Click on the "Get Form Here" button.
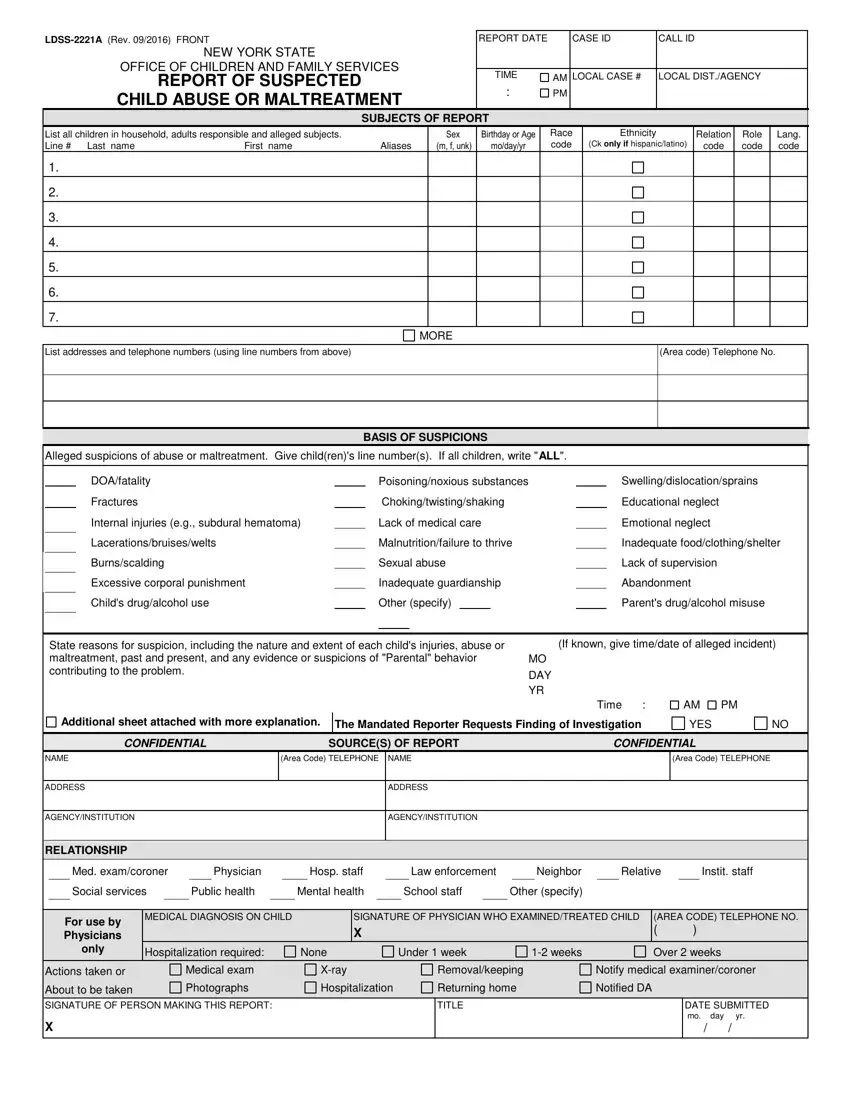
Step 2: The moment you enter our 2221a form acs editing page, you will notice all the options it is possible to take regarding your document within the upper menu.
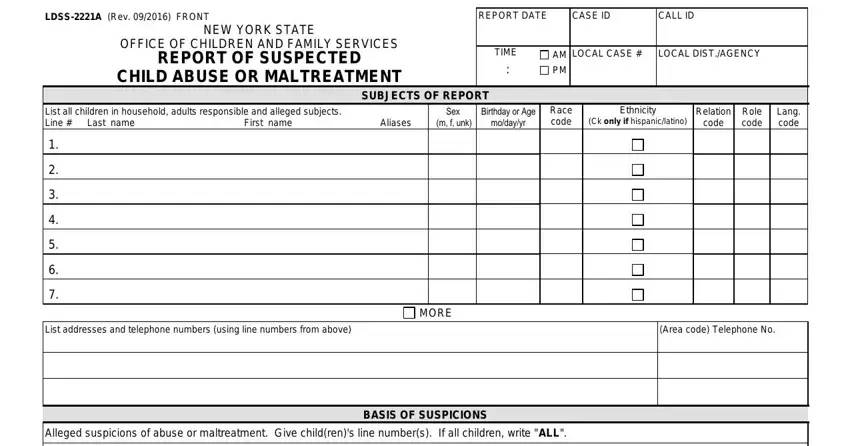
These particular parts will compose the PDF form that you'll be creating:
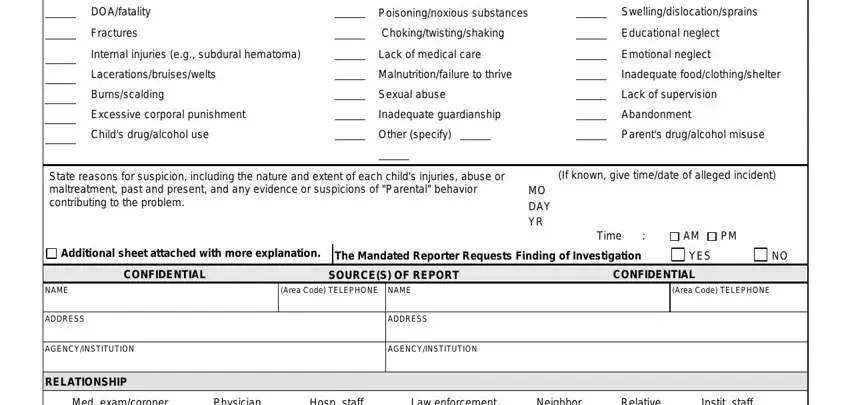
Make sure you write down the demanded information in the DOAfatality, Fractures, Internal injuries eg subdural, Poisoningnoxious substances, Lack of medical care, Swellingdislocationsprains, Educational neglect, Emotional neglect, Malnutritionfailure to thrive, Inadequate foodclothingshelter, Sexual abuse, Inadequate guardianship, Lack of supervision, Abandonment, and Other specify area.
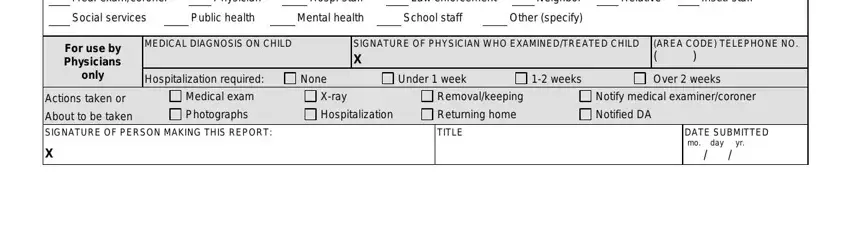
Write the significant particulars in RELATIONSHIP Med examcoroner, Physician, Hosp staff, Law enforcement, Neighbor, Relative, Instit staff, Public health, Mental health, School staff, Other specify, For use by Physicians only, Actions taken or, MEDICAL DIAGNOSIS ON CHILD, and SIGNATURE OF PHYSICIAN WHO section.
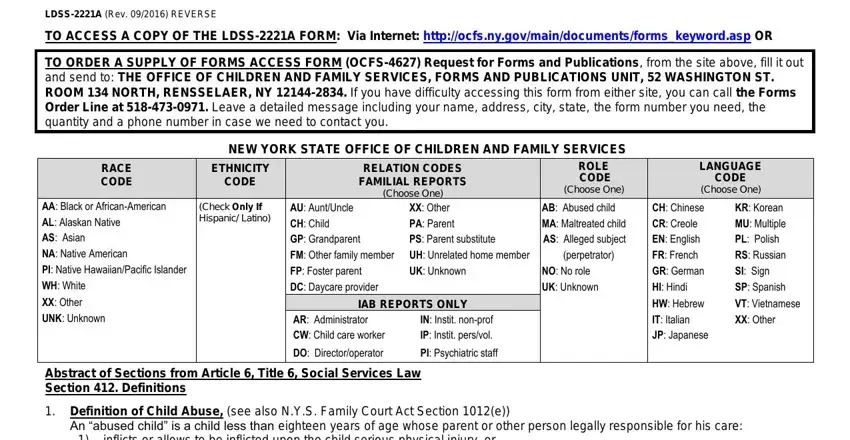
Feel free to identify the rights and responsibilities of the parties inside the LDSSA Rev REVERSE, TO ACCESS A COPY OF THE LDSSA FORM, TO ORDER A SUPPLY OF FORMS ACCESS, NEW YORK STATE OFFICE OF CHILDREN, ETHNICITY CODE, Check Only If Hispanic Latino, RACE CODE, AA Black or AfricanAmerican AL, RELATION CODES FAMILIAL REPORTS, AU AuntUncle XX Other CH Child PA, PS Parent substitute, UK Unknown, IAB REPORTS ONLY, AR Administrator CW Child care, and IN Instit nonprof IP Instit paragraph.
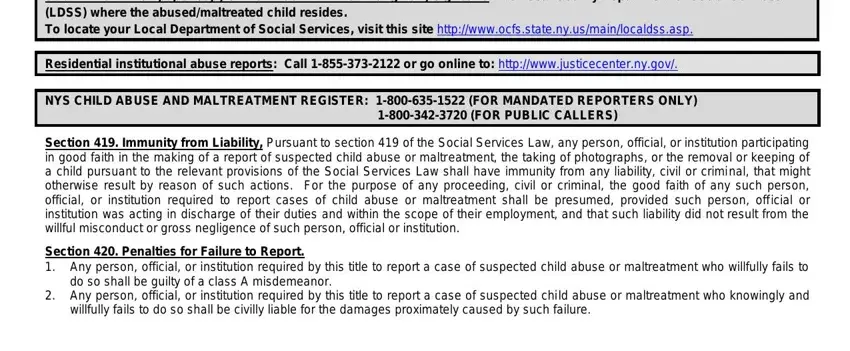
End by checking the following areas and completing them as required: Submit the written paper copy of, Residential institutional abuse, NYS CHILD ABUSE AND MALTREATMENT, Section Immunity from Liability, Section Penalties for Failure to, do so shall be guilty of a class A, Any person official or, and willfully fails to do so shall be.
Step 3: Press the Done button to make sure that your completed file could be transferred to any electronic device you pick out or forwarded to an email you indicate.
Step 4: You could make duplicates of your file toremain away from any potential future issues. Don't worry, we do not reveal or watch your data.
