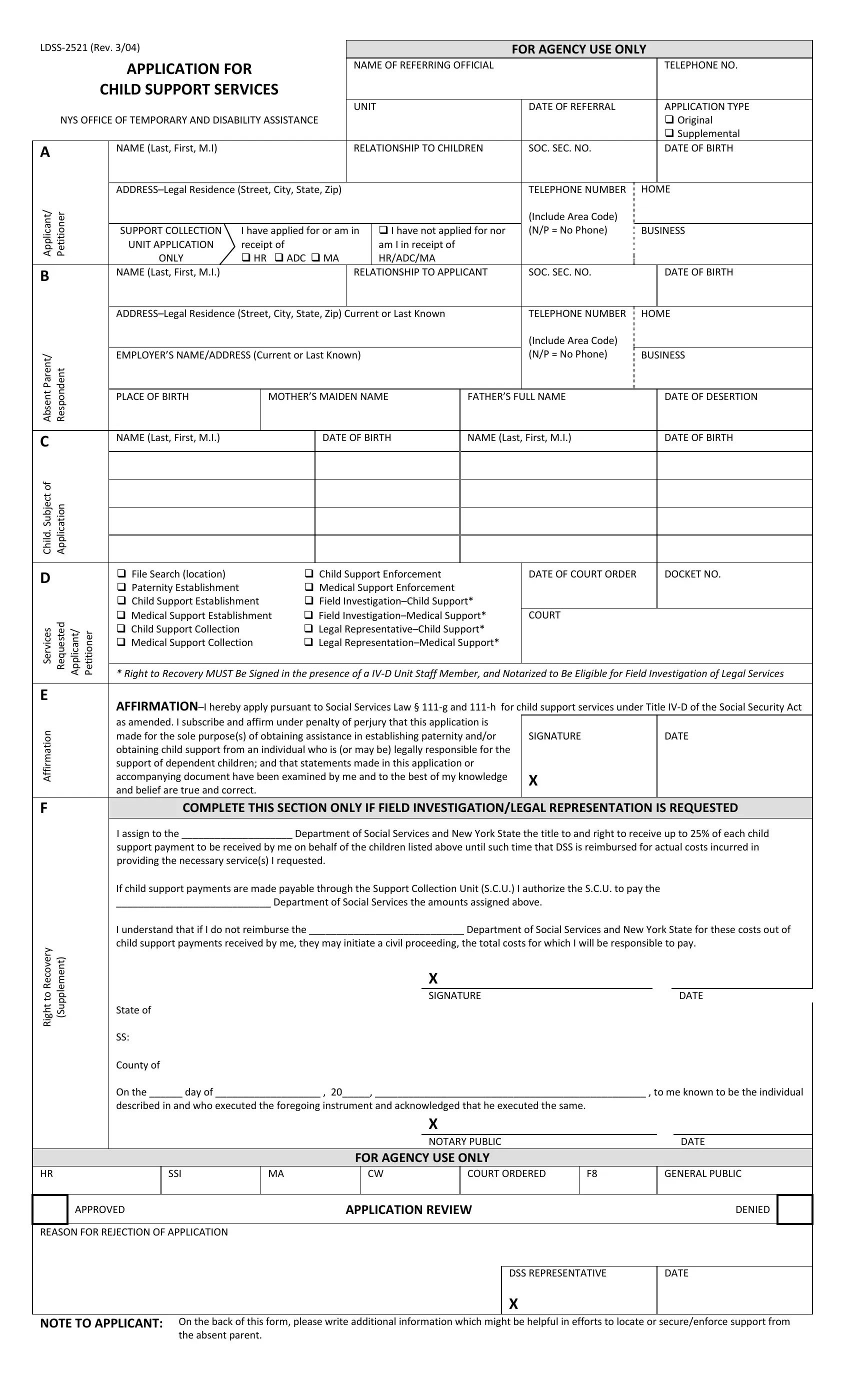
The LDSS-2521 form, revised in March 2004, serves as a critical document for individuals seeking child support services through the New York State Office of Temporary and Disability Assistance. Designed for agency use, this application encompasses several vital sections aimed at collecting comprehensive information to facilitate the establishment, enforcement, or modification of child support. It requires details about the applicant, including their relationship to the child or children involved, personal identification information, and residential address. The form also prompts the disclosure of information regarding the non-custodial parent or supposed absent parent, incorporating their employment details which are invaluable in the child support enforcement process. A noteworthy aspect of the LDSS-2521 is its affirmation section, where the applicant must assert, under the penalty of perjury, that the information provided is accurate and that the application is made with the intent to seek assistance in either establishing paternity and/or securing child support. Additionally, the form outlines a provision for assigning a portion of the child support received to cover the costs of services provided by the Department of Social Services and the State. The significance of this form lies not only in its role as an application but also as a legal document that outlines the rights and responsibilities of the applying party, underscoring the seriousness and legal implications of the child support process.
| Question | Answer |
|---|---|
| Form Name | Form Ldss 2521 |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | 111-g, NYS, New_York, LDSS-2521 |
|
|
|
|
|
|
|
|
|
|
|
FOR AGENCY USE ONLY |
||||||||||||
|
|
|
|
APPLICATION FOR |
|
|
|
NAME OF REFERRING OFFICIAL |
|
|
|
|
|
|
TELEPHONE NO. |
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
CHILD SUPPORT SERVICES |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
UNIT |
|
|
|
|
DATE OF REFERRAL |
|
|
APPLICATION TYPE |
|||||
|
|
NYS OFFICE OF TEMPORARY AND DISABILITY ASSISTANCE |
|
|
|
|
|
|
|
|
|
|
|
Original |
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Supplemental |
||
|
A |
|
|
NAME (Last, First, M.I) |
|
|
|
|
|
RELATIONSHIP TO CHILDREN |
|
SOC. SEC. NO. |
|
|
DATE OF BIRTH |
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
Applicant/ |
Petitioner |
|
|
|
|
|
TELEPHONE NUMBER |
HOME |
||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
(Include Area Code) |
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
SUPPORT COLLECTION |
I have applied for or am in |
|
I have not applied for nor |
|
(N/P = No Phone) |
BUSINESS |
|||||||||||||
|
|
|
|
UNIT APPLICATION |
receipt of |
|
|
|
|
|
am I in receipt of |
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
ONLY |
HR ADC MA |
|
HR/ADC/MA |
|
|
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||
|
B |
|
|
NAME (Last, First, M.I.) |
|
|
|
|
|
RELATIONSHIP TO APPLICANT |
|
SOC. SEC. NO. |
|
|
DATE OF BIRTH |
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
|
|
|
|
|
TELEPHONE NUMBER |
|
|
HOME |
||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
(Include Area Code) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
AbsentParent/ |
|
|
EMPLOYER’S NAME/ADDRESS (Current or Last Known) |
|
|
|
|
(N/P = No Phone) |
BUSINESS |
|||||||||||||
|
Respondent |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
PLACE OF BIRTH |
|
MOTHER’S MAIDEN NAME |
FATHER’S FULL NAME |
|
|
DATE OF DESERTION |
||||||||||||||||
|
|
|
|
|
|
|
|||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
C |
|
|
NAME (Last, First, M.I.) |
|
|
|
DATE OF BIRTH |
NAME (Last, First, M.I.) |
|
|
DATE OF BIRTH |
|||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Child. Subject of |
Application |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
D |
|
|
File Search (location) |
|
|
Child Support Enforcement |
|
|
DATE OF COURT ORDER |
|
|
DOCKET NO. |
||||||||||
|
|
|
Paternity Establishment |
|
|
Medical Support Enforcement |
|
|
|
|
|
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||
|
|
|
|
Child Support Establishment |
Field |
|
|
|
|
|
|
|
|
|
|||||||||
|
Services |
Requested Applicant/ Petitioner |
|
Medical Support Establishment |
Field |
|
COURT |
|
|
|
|
|
|||||||||||
|
|
Child Support Collection |
|
|
Legal |
|
|
|
|
|
|
|
|
|
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||
|
|
|
|
Medical Support Collection |
Legal |
|
|
|
|
|
|
|
|
|
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||
|
|
|
|
* Right to Recovery MUST Be Signed in the presence of a |
|||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
E |
|
|
||||||||||||||||||||
|
|
|
|
||||||||||||||||||||
|
Affirmation |
|
|
as amended. I subscribe and affirm under penalty of perjury that this application is |
|
|
|
|
|
|
|
|
|
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||
|
|
|
accompanying document have been examined by me and to the best of my knowledge |
|
|
|
|
|
|
|
|
|
|||||||||||
|
|
|
|
made for the sole purpose(s) of obtaining assistance in establishing paternity and/or |
|
SIGNATURE |
|
|
DATE |
||||||||||||||
|
|
|
|
obtaining child support from an individual who is (or may be) legally responsible for the |
|
|
|
|
|
|
|
|
|
||||||||||
|
|
|
|
support of dependent children; and that statements made in this application or |
|
|
|
|
|
|
|
|
|
||||||||||
|
|
|
|
and belief are true and correct. |
|
|
|
|
|
|
|
|
|
X |
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
F |
|
|
COMPLETE THIS SECTION ONLY IF FIELD INVESTIGATION/LEGAL REPRESENTATION IS REQUESTED |
|||||||||||||||||||
|
|
|
|
I assign to the ____________________ Department of Social Services and New York State the title to and right to receive up to 25% of each child |
|||||||||||||||||||
|
|
|
|
support payment to be received by me on behalf of the children listed above until such time that DSS is reimbursed for actual costs incurred in |
|||||||||||||||||||
|
|
|
|
providing the necessary service(s) I requested. |
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
|
|
|
If child support payments are made payable through the Support Collection Unit (S.C.U.) I authorize the S.C.U. to pay the |
|||||||||||||||||||
|
|
|
|
____________________________ Department of Social Services the amounts assigned above. |
|
|
|
|
|
||||||||||||||
|
|
|
|
I understand that if I do not reimburse the ____________________________ Department of Social Services and New York State for these costs out of |
|||||||||||||||||||
|
RecoverytoRight |
(Supplement) |
|
child support payments received by me, they may initiate a civil proceeding, the total costs for which I will be responsible to pay. |
|||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
X |
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
SIGNATURE |
|
|
|
|
|
|
|
|
DATE |
|
|
|
|
|
State of |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
SS: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
County of |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
On the ______ day of ___________________ , 20_____, _________________________________________________ , to me known to be the individual |
|||||||||||||||||||
|
|
|
|
described in and who executed the foregoing instrument and acknowledged that he executed the same. |
|
|
|
|
|
||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
X |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
NOTARY PUBLIC |
|
|
|
|
|
|
|
|
DATE |
|
|
|
|
|
|
|
|
|
|
|
FOR AGENCY USE ONLY |
|
|
|
|
|
|
|
|
|
||||
HR
SSI
MA
CW
COURT ORDERED
F8
GENERAL PUBLIC
APPROVED |
APPLICATION REVIEW |
DENIED |
REASON FOR REJECTION OF APPLICATION
DSS REPRESENTATIVE
X
DATE
NOTE TO APPLICANT: On the back of this form, please write additional information which might be helpful in efforts to locate or secure/enforce support from the absent parent.