Understanding the LDSS-3113 form is crucial for individuals undergoing a hysterectomy under the New York State Medicaid program. This document serves as a formal acknowledgment that the patient has been fully informed about the nature and implications of a hysterectomy, a surgical procedure that results in the inability to become pregnant or bear children. The form is divided into two parts, with the first part requiring the recipient's acknowledgment of understanding the permanent consequences of the procedure, along with the surgeon's certification that the surgery is being performed purely for medical reasons, not for the purpose of sterilization. The second part of the form acts as a waiver, used in specific circumstances such as when the surgery is conducted in a life-threatening emergency, or the recipient was already unable to reproduce before the surgery was planned. It highlights the importance of informed consent in the medical field, ensuring that patients are fully aware of the significant outcomes associated with such a procedure, and that surgeons comply with regulatory requirements when performing surgeries funded by Medicaid.
| Question | Answer |
|---|---|
| Form Name | Form Ldss 3113 |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | ldss 3113 form, RECIPIENTS, secondarily, anesthesiologist |
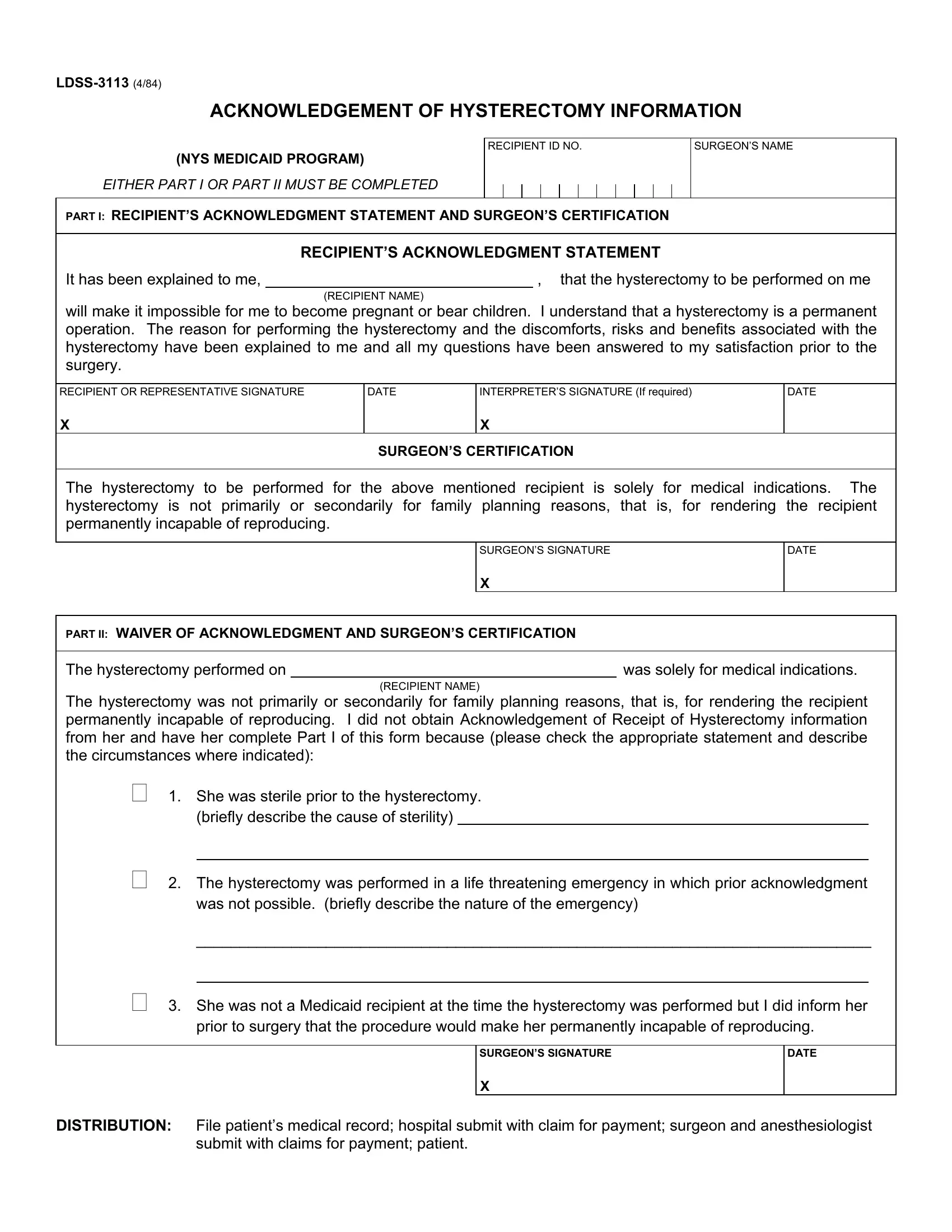
ACKNOWLEDGEMENT OF HYSTERECTOMY INFORMATION
(NYS MEDICAID PROGRAM)
EITHER PART I OR PART II MUST BE COMPLETED
RECIPIENT ID NO.
SURGEON’S NAME
PART I: RECIPIENT’S ACKNOWLEDGMENT STATEMENT AND SURGEON’S CERTIFICATION
RECIPIENT’S ACKNOWLEDGMENT STATEMENT
It has been explained to me, |
|
, that the hysterectomy to be performed on me |
(RECIPIENT NAME)
will make it impossible for me to become pregnant or bear children. I understand that a hysterectomy is a permanent operation. The reason for performing the hysterectomy and the discomforts, risks and benefits associated with the hysterectomy have been explained to me and all my questions have been answered to my satisfaction prior to the surgery.
RECIPIENT OR REPRESENTATIVE SIGNATURE
X
DATE
INTERPRETER’S SIGNATURE (If required)
X
DATE
SURGEON’S CERTIFICATION
The hysterectomy to be performed for the above mentioned recipient is solely for medical indications. The hysterectomy is not primarily or secondarily for family planning reasons, that is, for rendering the recipient permanently incapable of reproducing.
SURGEON’S SIGNATURE
DATE
X
PART II: WAIVER OF ACKNOWLEDGMENT AND SURGEON’S CERTIFICATION
The hysterectomy performed on |
|
was solely for medical indications. |
(RECIPIENT NAME)
The hysterectomy was not primarily or secondarily for family planning reasons, that is, for rendering the recipient permanently incapable of reproducing. I did not obtain Acknowledgement of Receipt of Hysterectomy information from her and have her complete Part I of this form because (please check the appropriate statement and describe the circumstances where indicated):
1.She was sterile prior to the hysterectomy. (briefly describe the cause of sterility)
2.The hysterectomy was performed in a life threatening emergency in which prior acknowledgment was not possible. (briefly describe the nature of the emergency)
______________________________________________________________________________
3. She was not a Medicaid recipient at the time the hysterectomy was performed but I did inform her prior to surgery that the procedure would make her permanently incapable of reproducing.
SURGEON’S SIGNATURE
DATE
X
DISTRIBUTION: File patient’s medical record; hospital submit with claim for payment; surgeon and anesthesiologist submit with claims for payment; patient.