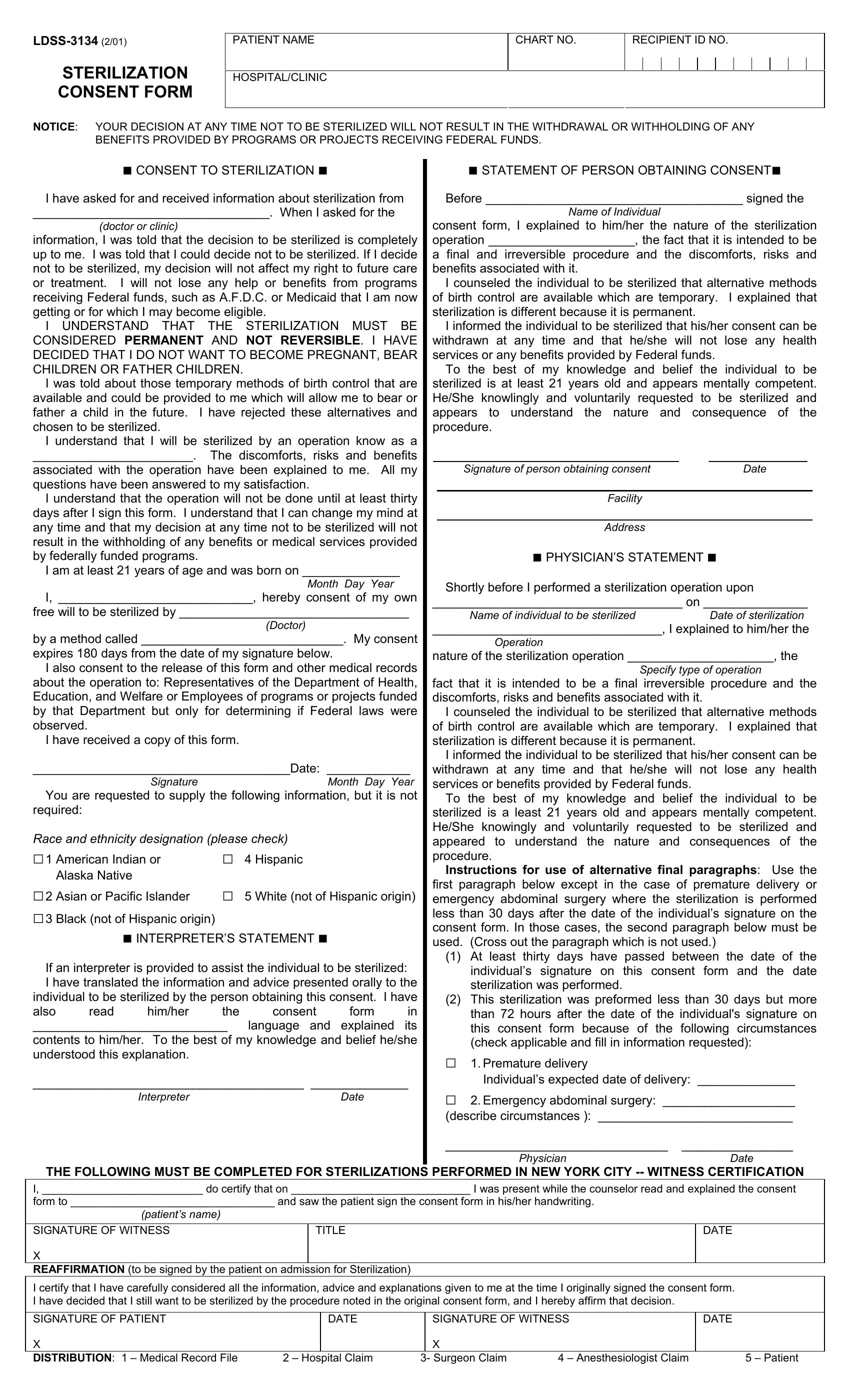
When individuals make the significant decision to undergo sterilization, they are presented with the LDSS-3134 form, a document that plays a crucial role in the process. This form, mandated for use in settings that receive federal funding, is not just a bureaucratic step but a safeguard for the rights and well-being of the patient. Its contents cover a broad spectrum, emphasizing the voluntary nature of sterilization, the irreversible aspect of the procedure, and the comprehensive explanation and counseling that patients must receive before making their decision. Patients are reassured that their access to benefits and medical services will not be impacted by their choice regarding sterilization. Detailed within the form are also provisions for consent expiration, requirements for interpreter assistance for non-English speakers, and a mandatory waiting period before the procedure can be conducted. This ensures that patients have ample time to consider their decision. In addition, the form gathers demographic information for statistical purposes, while strictly adhering to privacy and consent standards set by federal regulations. The LDSS-3134 Sterilization Consent Form encapsulates a confluence of medical, ethical, and legal considerations, designed to protect patient rights while ensuring informed consent for a life-altering medical procedure.
| Question | Answer |
|---|---|
| Form Name | Form Ldss 3134 |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | dss 3134 form, form ldss 3134, how to fill out ldss 3134, nys sterilization consent form |
