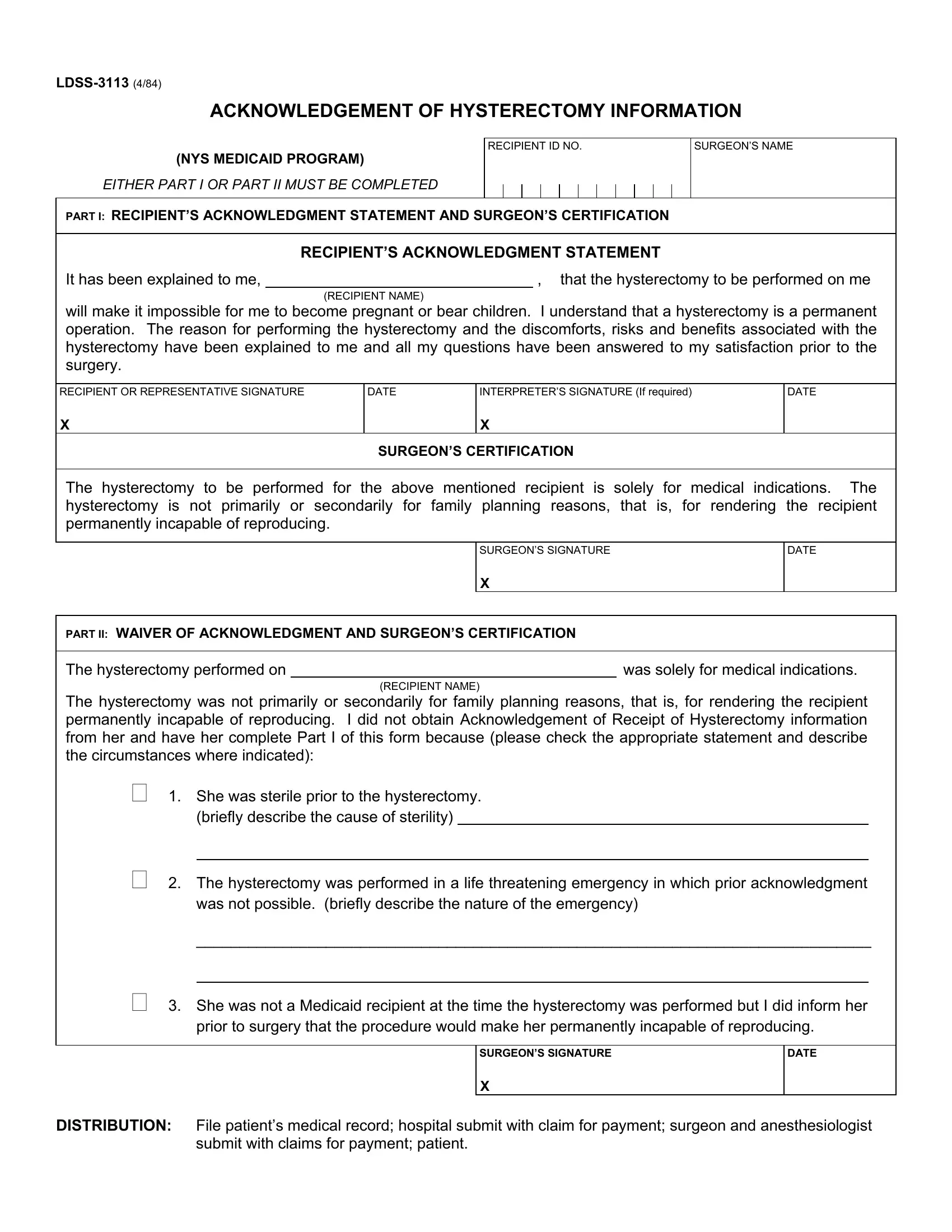
Understanding the LDSS-3113 form is crucial for individuals undergoing a hysterectomy under the New York State Medicaid program. This document serves as a formal acknowledgment that the patient has been fully informed about the nature and implications of a hysterectomy, a surgical procedure that results in the inability to become pregnant or bear children. The form is divided into two parts, with the first part requiring the recipient's acknowledgment of understanding the permanent consequences of the procedure, along with the surgeon's certification that the surgery is being performed purely for medical reasons, not for the purpose of sterilization. The second part of the form acts as a waiver, used in specific circumstances such as when the surgery is conducted in a life-threatening emergency, or the recipient was already unable to reproduce before the surgery was planned. It highlights the importance of informed consent in the medical field, ensuring that patients are fully aware of the significant outcomes associated with such a procedure, and that surgeons comply with regulatory requirements when performing surgeries funded by Medicaid.
| Question | Answer |
|---|---|
| Form Name | Form Ldss 3113 |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | ldss 3113 form, RECIPIENTS, secondarily, anesthesiologist |
