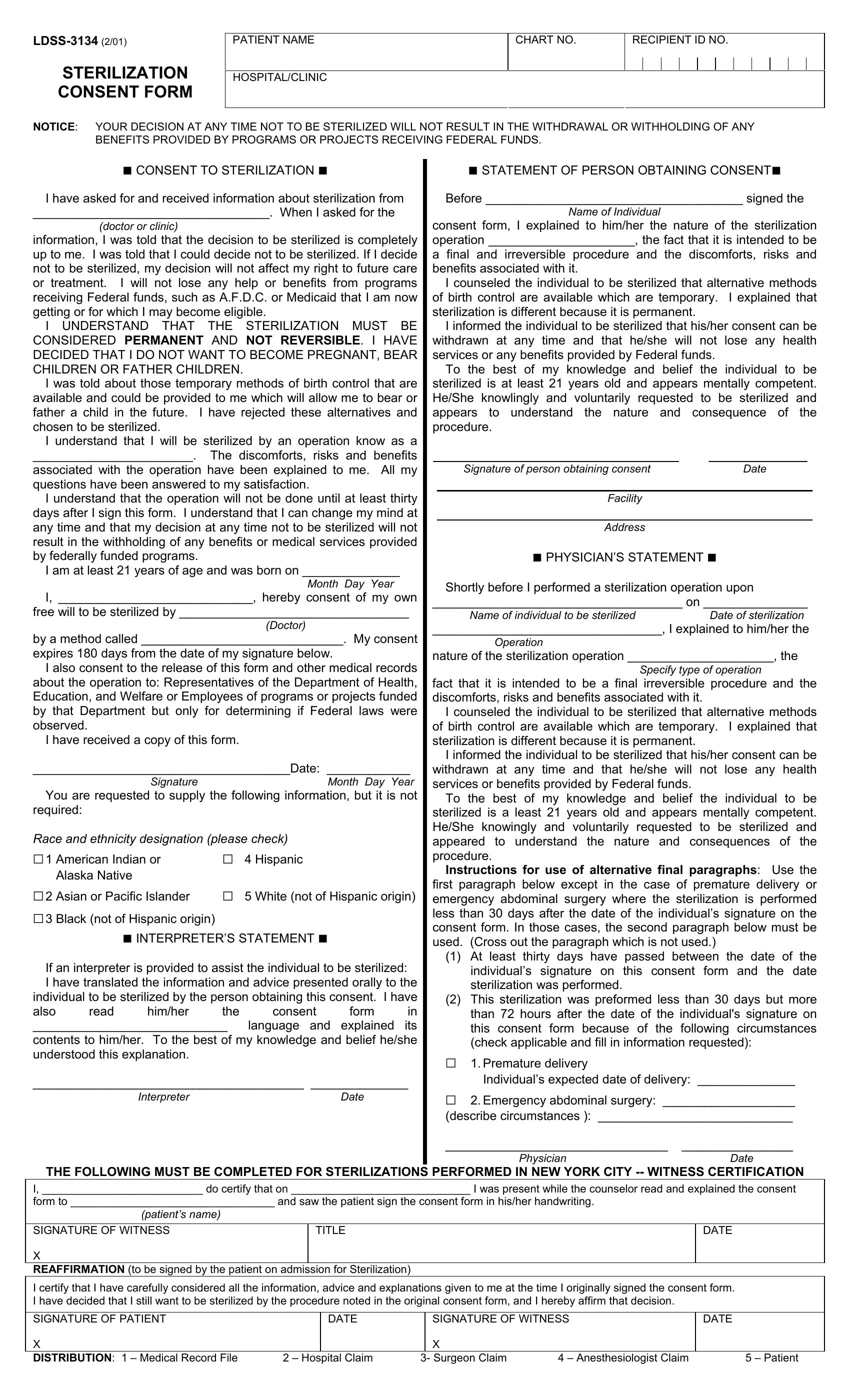
When individuals make the significant decision to undergo sterilization, they are presented with the LDSS-3134 form, a document that plays a crucial role in the process. This form, mandated for use in settings that receive federal funding, is not just a bureaucratic step but a safeguard for the rights and well-being of the patient. Its contents cover a broad spectrum, emphasizing the voluntary nature of sterilization, the irreversible aspect of the procedure, and the comprehensive explanation and counseling that patients must receive before making their decision. Patients are reassured that their access to benefits and medical services will not be impacted by their choice regarding sterilization. Detailed within the form are also provisions for consent expiration, requirements for interpreter assistance for non-English speakers, and a mandatory waiting period before the procedure can be conducted. This ensures that patients have ample time to consider their decision. In addition, the form gathers demographic information for statistical purposes, while strictly adhering to privacy and consent standards set by federal regulations. The LDSS-3134 Sterilization Consent Form encapsulates a confluence of medical, ethical, and legal considerations, designed to protect patient rights while ensuring informed consent for a life-altering medical procedure.
| Question | Answer |
|---|---|
| Form Name | Form Ldss 3134 |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | dss 3134 form, form ldss 3134, how to fill out ldss 3134, nys sterilization consent form |
STERILIZATION CONSENT FORM
PATIENT NAME |
CHART NO. |
RECIPIENT ID NO. |
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
HOSPITAL/CLINIC
NOTICE: YOUR DECISION AT ANY TIME NOT TO BE STERILIZED WILL NOT RESULT IN THE WITHDRAWAL OR WITHHOLDING OF ANY BENEFITS PROVIDED BY PROGRAMS OR PROJECTS RECEIVING FEDERAL FUNDS.
■ CONSENT TO STERILIZATION ■
I have asked for and received information about sterilization from
__________________________________. When I asked for the
(doctor or clinic)
information, I was told that the decision to be sterilized is completely up to me. I was told that I could decide not to be sterilized. If I decide not to be sterilized, my decision will not affect my right to future care or treatment. I will not lose any help or benefits from programs receiving Federal funds, such as A.F.D.C. or Medicaid that I am now getting or for which I may become eligible.
I UNDERSTAND THAT THE STERILIZATION MUST BE CONSIDERED PERMANENT AND NOT REVERSIBLE. I HAVE DECIDED THAT I DO NOT WANT TO BECOME PREGNANT, BEAR CHILDREN OR FATHER CHILDREN.
I was told about those temporary methods of birth control that are available and could be provided to me which will allow me to bear or father a child in the future. I have rejected these alternatives and chosen to be sterilized.
I understand that I will be sterilized by an operation know as a
_______________________. The discomforts, risks and benefits
associated with the operation have been explained to me. All my questions have been answered to my satisfaction.
I understand that the operation will not be done until at least thirty days after I sign this form. I understand that I can change my mind at any time and that my decision at any time not to be sterilized will not result in the withholding of any benefits or medical services provided by federally funded programs.
I am at least 21 years of age and was born on ______________
Month Day Year
I, ____________________________, hereby consent of my own
free will to be sterilized by _________________________________
(Doctor)
by a method called _____________________________. My consent
expires 180 days from the date of my signature below.
I also consent to the release of this form and other medical records about the operation to: Representatives of the Department of Health, Education, and Welfare or Employees of programs or projects funded by that Department but only for determining if Federal laws were observed.
I have received a copy of this form.
_____________________________________Date: ____________
Signature |
Month Day Year |
You are requested to supply the following information, but it is not required:
Race and ethnicity designation (please check)
□1 |
American Indian or |
□ |
4 |
Hispanic |
□2 |
Alaska Native |
□ |
|
|
Asian or Pacific Islander |
5 |
White (not of Hispanic origin) |
□3 Black (not of Hispanic origin)
■INTERPRETER’S STATEMENT ■
If an interpreter is provided to assist the individual to be sterilized: I have translated the information and advice presented orally to the individual to be sterilized by the person obtaining this consent. I have also read him/her the consent form in
____________________________ language and explained its
contents to him/her. To the best of my knowledge and belief he/she understood this explanation.
_______________________________________ ______________
Interpreter |
Date |
■ STATEMENT OF PERSON OBTAINING CONSENT■
Before _____________________________________ signed the
Name of Individual
consent form, I explained to him/her the nature of the sterilization operation _____________________, the fact that it is intended to be
a final and irreversible procedure and the discomforts, risks and benefits associated with it.
I counseled the individual to be sterilized that alternative methods of birth control are available which are temporary. I explained that sterilization is different because it is permanent.
I informed the individual to be sterilized that his/her consent can be withdrawn at any time and that he/she will not lose any health services or any benefits provided by Federal funds.
To the best of my knowledge and belief the individual to be sterilized is at least 21 years old and appears mentally competent. He/She knowlingly and voluntarily requested to be sterilized and appears to understand the nature and consequence of the procedure.
Signature of person obtaining consent |
Date |
Facility
Address
■ PHYSICIAN’S STATEMENT ■
Shortly before I performed a sterilization operation upon
____________________________________ on _______________
Name of individual to be sterilized Date of sterilization
_________________________________, I explained to him/her the
Operation
nature of the sterilization operation _____________________, the
Specify type of operation
fact that it is intended to be a final irreversible procedure and the discomforts, risks and benefits associated with it.
I counseled the individual to be sterilized that alternative methods of birth control are available which are temporary. I explained that sterilization is different because it is permanent.
I informed the individual to be sterilized that his/her consent can be withdrawn at any time and that he/she will not lose any health services or benefits provided by Federal funds.
To the best of my knowledge and belief the individual to be sterilized is a least 21 years old and appears mentally competent. He/She knowingly and voluntarily requested to be sterilized and appeared to understand the nature and consequences of the procedure.
Instructions for use of alternative final paragraphs: Use the first paragraph below except in the case of premature delivery or emergency abdominal surgery where the sterilization is performed less than 30 days after the date of the individual’s signature on the consent form. In those cases, the second paragraph below must be used. (Cross out the paragraph which is not used.)
(1)At least thirty days have passed between the date of the individual’s signature on this consent form and the date sterilization was performed.
(2)This sterilization was preformed less than 30 days but more than 72 hours after the date of the individual's signature on this consent form because of the following circumstances (check applicable and fill in information requested):
□1. Premature delivery
Individual’s expected date of delivery: ______________
□2. Emergency abdominal surgery: ___________________
(describe circumstances ): ____________________________
________________________________ ________________
PhysicianDate
THE FOLLOWING MUST BE COMPLETED FOR STERILIZATIONS PERFORMED IN NEW YORK CITY
I, __________________________ do certify that on _____________________________ I was present while the counselor read and explained the consent
form to _________________________________ and saw the patient sign the consent form in his/her handwriting.
(patient’s name)
SIGNATURE OF WITNESS |
TITLE |
X
REAFFIRMATION (to be signed by the patient on admission for Sterilization)
DATE
I certify that I have carefully considered all the information, advice and explanations given to me at the time I originally signed the consent form. I have decided that I still want to be sterilized by the procedure noted in the original consent form, and I hereby affirm that decision.
SIGNATURE OF PATIENT |
|
DATE |
|
SIGNATURE OF WITNESS |
DATE |
|
X |
|
|
|
X |
|
|
DISTRIBUTION: 1 – Medical Record File |
2 – Hospital Claim |
3- Surgeon Claim |
4 – Anesthesiologist Claim |
5 – Patient |
||