Navigating through the process of applying for Food Stamp benefits in New York State involves understanding and completing the LDSS-4826 form, an essential document furnished by the New York State Office of Temporary and Disability Assistance. This comprehensive form serves as the foundation for applicants to detail their personal information, living arrangements, income, resources, and any significant changes that may impact their eligibility for assistance. With sections dedicated to capturing detailed household composition, including each member's age, income, and relationship to the applicant, the form is designed to ensure applicants provide a full picture of their financial situation. Furthermore, it addresses critical areas such as citizenship status, disabilities, and whether any household members are fleeing law enforcement, which are crucial for determining eligibility. The form also delves into the specifics of living expenses, including rent or mortgage, utilities, and child care costs, offering a holistic view of the applicant's financial obligations. Compliance with the food stamp program's regulations is underscored through stern warnings against fraud and the requirement for honest disclosure, emphasizing the legal implications of providing false information. Moreover, the LDSS-4826 form outlines the necessity of reporting any changes in household circumstances promptly, ensuring that the assistance provided aligns with current needs. Designed to facilitate a thorough evaluation by the Department of Social Services, this form plays a pivotal role in the application process, guiding both applicants and caseworkers through the meticulous assessment of eligibility for Food Stamp benefits.
| Question | Answer |
|---|---|
| Form Name | Form Ldss 4826 |
| Form Length | 5 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 1 min 15 sec |
| Other names | recertification, USDA, Whitten, TDD |
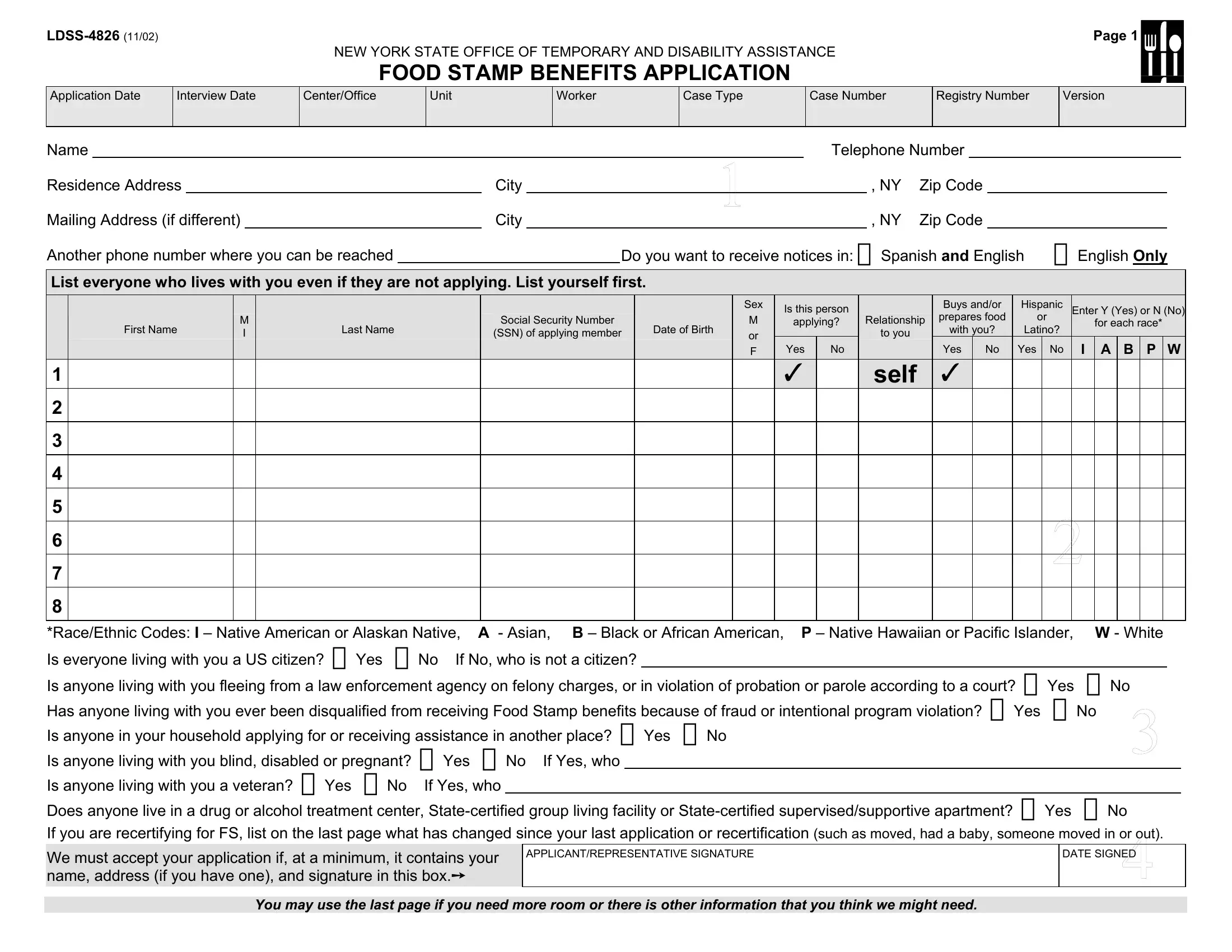
Page 1 |
NEW YORK STATE OFFICE OF TEMPORARY AND DISABILITY ASSISTANCE
FOOD STAMP BENEFITS APPLICATION
Application Date
Interview Date
Center/Office
Unit
Worker
Case Type
Case Number
Registry Number
Version
Name |
|
|
|
|
Telephone Number |
|
|
|
||||||
Residence Address |
|
City |
|
|
|
, NY |
Zip Code |
|
|
|
||||
Mailing Address (if different) |
|
City |
|
|
|
, NY |
Zip Code |
|
|
|
||||
Another phone number where you can be reached |
|
|
|
Do you want to receive notices in: Spanish and English |
English Only |
|||||||||
List everyone who lives with you even if they are not applying. List yourself first.
1
2
3
4
5
6
7
8
|
|
|
|
|
Sex |
Is this person |
|
Buys and/or |
Hispanic |
Enter Y (Yes) or N (No) |
||||||||
|
M |
|
Social Security Number |
|
M |
Relationship |
prepares food |
or |
||||||||||
|
|
|
||||||||||||||||
|
|
|
applying? |
|
for each race* |
|||||||||||||
First Name |
Last Name |
Date of Birth |
with you? |
Latino? |
||||||||||||||
I |
(SSN) of applying member |
or |
|
|
to you |
|
|
|
|
|
||||||||
|
|
|
|
|
Yes |
No |
|
Yes |
No |
Yes |
No |
I |
A |
B |
P |
W |
||
|
|
|
|
|
|
|||||||||||||
|
|
|
|
|
F |
|
||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
self
*Race/Ethnic Codes: I – Native American or Alaskan Native, |
A - Asian, B – Black or African American, P – Native Hawaiian or Pacific Islander, |
W - White |
|
|||||
Is everyone living with you a US citizen? Yes No If No, who is not a citizen? |
|
|
|
|
||||
Is anyone living with you fleeing from a law enforcement agency on felony charges, or in violation of probation or parole according to a court? |
Yes |
No |
|
|||||
Has anyone living with you ever been disqualified from receiving Food Stamp benefits because of fraud or intentional program violation? Yes No |
|
|||||||
Is anyone in your household applying for or receiving assistance in another place? Yes No |
|
|
|
|||||
Is anyone living with you blind, disabled or pregnant? |
Yes |
No If Yes, who |
|
|
|
|
||
Is anyone living with you a veteran? Yes No |
If Yes, who |
|
|
|
|
|||
Does anyone live in a drug or alcohol treatment center, |
Yes |
No |
|
|||||
If you are recertifying for FS, list on the last page what has changed since your last application or recertification
We must accept your application if, at a minimum, it contains your name, address (if you have one), and signature in this box.
APPLICANT/REPRESENTATIVE SIGNATURE
You may use the last page if you need more room or there is other information that you think we might need.
Page 2 |
INCOME
List ALL the income of anyone living with you. This includes, but is not limited to wages, income from
Name of Person Receiving Income
Source of Income
How Often is it Received?
(for example, weekly,
Gross Amount Received Before Deductions
Does anyone living with you have child/dependent care costs related to employment or training? Yes No If Yes, who.
Amount paid $ ____________ . How often paid (e.g., weekly, monthly) _________________________ .
Has anyone living with you changed or quit jobs or reduced any form of income in the last 30 days – including reduced work hours or income? Yes No
Does anyone living with you have any potential income that has not yet been received? Yes No |
If Yes, explain on last page. |
|
|
|
|||||||
Does anyone living with you receive a Personal Needs Allowance (PNA) or a Meal Allowance? Yes |
No If Yes, who |
|
|
. |
|||||||
Has anyone in your household set aside any income under “PASS: Plan To Achieve Self Support” approved by the Social Security Administration? Yes |
No |
||||||||||
If Yes, who |
|
|
. |
|
|
|
|
|
|
|
|
Is anyone living with you participating in a strike? Yes |
No If Yes, who |
|
|
|
. |
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
RESOURCES |
|
|
|
|
|
|
How much money does everyone applying have? (For example, on your person; in your home, in checking and savings accounts, or other locations, including jointly held accounts) |
|||||||||||
$______________ Belongs to |
|
|
|
|
|
. |
|
|
|
|
|
Other financial assets? (For example, stocks, bonds, retirement accounts, savings bonds, mutual funds, IRAs, trust funds, money market certificates) Yes No |
|
|
|
||||||||
If Yes, amount $_______________ Type ________________________________ Owner _________________________________ .
How many cars, trucks or other vehicles do you have? ____ #1 Year ______ Make ________________ Model _______________ Owner __________________ Used for: __________________
#2 Year ______ Make ________________ Model _________________ Owner __________________ Used for: _________________________
Do you or anyone applying own any property including your own home? Yes No List ________________________________ Owner ________________________
Has anyone applying sold, given away or transferred cash or property in the last three months to qualify for Food Stamp benefits? Yes No
LIVING ARRANGEMENTS AND EXPENSES
Check all the descriptions that apply to your household:
Own home or paying for home Renting Migrant/seasonal farm worker No permanent residence Live with relatives or friends
List your expenses: Monthly rent or mortgage payment $ _______________ Tax on home per year $ _______________ Insurance on home per year $ _______________ .
Monthly heating/cooling cost $_______________ Specify type of heating: Gas Electric Oil Wood |
Coal Other (list) _______________________ . |
Monthly utilities (other than heating/cooling) $______________ Other (for example, garbage/trash, water, initial installation of utilities) $___________________ . |
|
Monthly telephone expense $__________________ . |
|
Do you have an air conditioner or have central air conditioning? Yes No |
|
Does anyone living with you pay any of these expenses for you (including Section 8 or other subsidy program)? Yes |
No If yes, who ___________________________________ . |
Does anyone living with you pay
Name(s) of child(ren) support is being paid for _____________________________________________________________________________
Payment amount $__________________ Frequency of payments (for example, weekly,
Does anyone living with you have medical bills? Yes No If yes, list on the last page what they are for, how much and who is responsible for payment.
Is anyone living with you (16 years old or older) enrolled in school or training? Yes No If yes, who _________________________ Where ______________________
You may use the last page if you need more room or there is other information that you think we might need.
Page 3 |
|
|
READ THE IMPORTANT INFORMATION BELOW AND SIGN AT THE BOTTOM |
FOOD STAMP BENEFITS (FS) PENALTY WARNING – Any information you provide in connection with your application for Food Stamp Benefits will be subject to verification by Federal, State and local officials. If any information is incorrect, you may be denied FS. You may be subject to criminal prosecution for knowingly providing incorrect information.
You will never be able to get FS again if you are found guilty in a court of law for the second time of buying or selling controlled substances (illegal drugs or certain drugs for which a doctor’s prescription is required) in exchange for FS; or found guilty in a court of law of selling or getting firearms, ammunition or explosives in exchange for FS; or found guilty in a court of law of trafficking in FS worth $500 or more. Trafficking includes the illegal use, transfer, acquisition, alteration or possession of FS, authorization cards or access devices; or found guilty of committing a third Intentional Program Violation (IPV).
You will not be able to get FS for two years if you are found guilty in a court of law for the first time of buying or selling controlled substances (illegal drugs or certain drugs for which a doctor’s prescription is required) in exchange for FS.
If you have committed your: First IPV, you will not be able to get FS for one year. Second IPV, you will not be able to get FS for two years.
A court could also bar you from receiving Food Stamp Benefits for an additional 18 months. If you make a false statement about who you are or where you live in order to get multiple FS, you will not be able to get FS for ten years (or permanently if this is the third IPV).
You may be found guilty of an Intentional Program Violation if you make a false or misleading statement, or misrepresent, conceal or withhold facts; or commit any act that constitutes a violation of Federal or State law for the purpose of using, presenting, transferring, acquiring, receiving, possessing or trafficking of coupons, authorization cards or reusable documents used as part of the Electronic Benefit Transfer (EBT) system.
You could also be fined up to $250,000, sent to jail for up to 20 years, or both.
CONSENT – I understand that by signing this application form I agree to any investigation made by the Department of Social Services to verify or confirm the information I have given or any other investigation made by them in connection with my request for FS benefits. If additional information is requested, I will provide it. I will also cooperate with State and Federal personnel in a Food Stamp Quality Control Review.
SUA INFORMATION – I understand that Food Stamp recipients are categorically income eligible for the Home Energy Assistance Program (HEAP). If I am not included in the annual automatic HEAP payment process for certain FS recipients, I intend to apply for a benefit within the next 12 months. If I decide not to apply for HEAP within the next 12 months, I will let my worker know.
CHANGES – I agree to inform the agency promptly of any change in my needs, income, property, living arrangement or address to the best of my knowledge or belief.
REQUIREMENT TO REPORT/VERIFY HOUSEHOLD EXPENSES – I understand that my household must report child care and utility expenses in order to get a Food Stamp deduction for these expenses. I further understand that my household must report and verify rent/mortgage payments, property taxes, insurance, medical expenses and child support paid to a
I understand that failure to report/verify the above expenses will be seen as a statement by my household that I/we do not want to receive a deduction for those unreported/unverified expenses. A deduction for these expenses may make me eligible for FS or may increase my FS benefits. I understand that I may report/verify these expenses at any time in the future. This deduction would then be applied to the calculation of FS benefits in future months in accordance with the rules for change reporting.
PRIVACY ACT STATEMENT – COLLECTION AND USE OF SOCIAL SECURITY NUMBER (SSN) – The collection of SSN’s is authorized for each household member with respect to Food Stamp Benefits pursuant to the Food Stamp Act of 1977 (as amended, 7 US Code
If you do not have an SSN and need to get one, the information you give to the social service district may be used to get one for you.
CERTIFICATION OR CITIZENSHIP/ALIEN STATUS FOR FOOD STAMPS – I swear and affirm under penalties of perjury, that all household members except ______________________
are United States (U.S.) citizens or nationals or persons with satisfactory immigration status. I understand that information about my Food Stamp household will be submitted to the Immigration and Naturalization Service (INS) for verification of immigration status, if applicable. I further understand that the use or disclosure of information about household members including myself who are applying for or receiving FS is restricted to persons and organizations directly connected with the verification of immigration status and the administration or enforcement of provisions of the Food Stamp Program. I also understand that information received from the INS may affect my household’s eligibility and level of benefits.
AUTHORIZED REPRESENTATIVE – You can authorize someone who knows your household circumstances to apply for FS for you. If you do, have them sign in the signature section at the bottom of this page. You can also authorize someone outside your household to get FS for you and to use them to buy food for you. If you would like to authorize someone, print the person’s name, address and phone number below.
CERTIFICATION: I swear and/or affirm under the penalties of perjury that the information I have given or will give to the local Social Services district is correct.
APPLICANT/REPRESENTATIVE SIGNATURE
X
DATE SIGNED
HUSBAND/WIFE SIGNATURE
X
DATE SIGNED
IF APPLYING FOR SOMEONE ELSE AS AN AUTHORIZED REPRESENTATIVE, PRINT YOUR NAME AND ADDRESS HERE. YOU MAY ALSO VOLUNTARILY PRINT YOUR TELEPHONE NUMBER.
Name ___________________________________________ Address _____________________________________________________________________________ Phone _______________
Page 4 |
|
Use this area for additional information: |
|
Who: ________________________________________Explanation: |
|
Who: ________________________________________Explanation:
Who: ________________________________________Explanation:
I CONSENT TO WITHDRAW MY APPLICATION. I understand that I may reapply at any time.
SIGNATURE
DATE
For Agency Use Only
Eligibility Determined by __________________________________________________________________________ Date ___________________________
Signature of Person Who Obtained Eligibility Information: ___________________________________________________________ Date _________________________
Employed by: Social Services District Provider Agency
(Specify) ______________________________________________________________________________________
Reason _____/_____/______ |
Withdrawal |
Denial |
Recert. Closing |
Eligibility Approved by ___________________________________________________________________________ Date _______________________
FS Authorization Period: From ______________________ To ______________________
Comments: