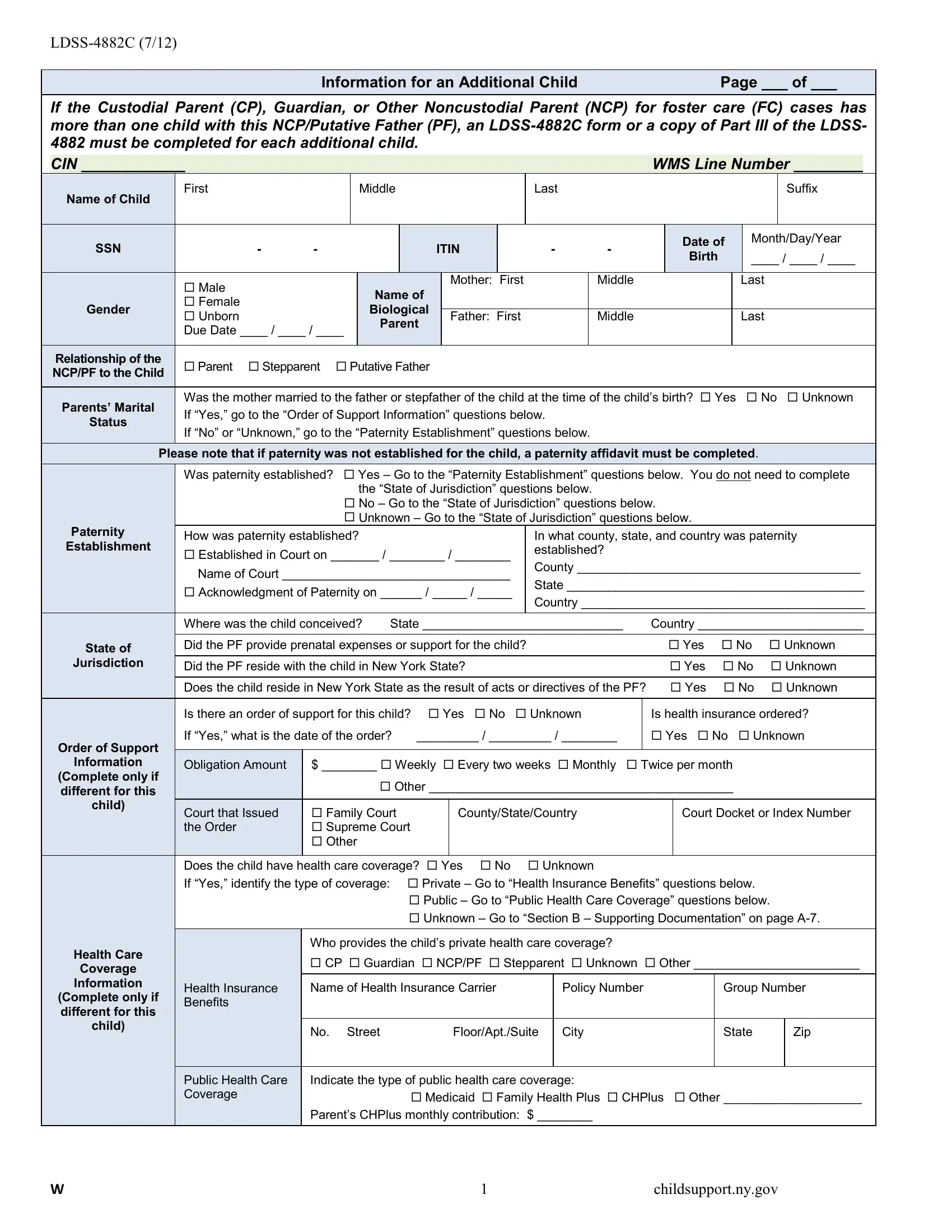
In today's complex family environments, effective management of child support and understanding the intricacies involved becomes imperative, especially when multiple children are concerned within the same case parameters. The LDSS-4882C form, a critical document released in July 2012, stands as an essential tool for custodial parents, guardians, and noncustodial parents in scenarios involving foster care. This form ensures that each child's unique needs and circumstances are thoroughly documented and considered in child support proceedings. It requires detailed information about additional children when a custodial parent (CP), guardian, or noncustodial parent (NCP) has more than one child with the same NCP or putative father (PF), demanding a separate completion for each child. The form encompasses a wide range of data, including but not limited to the child’s personal information, paternity establishment queries, state of jurisdiction considerations, order of support information, and specific sections on health care coverage. For foster care cases, there's an exclusive section that must be completed by the Commissioner or Designee, highlighting the form's versatility and the comprehensive nature of the data it seeks to collect to ensure the welfare of the child or children in question. Through the structured collection of this information, the form plays a pivotal role in facilitating the accurate assessment and enforcement of support obligations, thereby aiming to safeguard the best interests of each child involved.
| Question | Answer |
|---|---|
| Form Name | Form Ldss 4882C |
| Form Length | 2 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 30 sec |
| Other names | nys form ldss 486t, ldss 4882c fillable form, ldss 486t, heap form ldss 3829 |
