STATE OF CALIFORNIA - HEALTH AND HUMAN SERVICES AGENCY |
CALIFORNIA DEPARTMENT OF SOCIAL SERVICES |
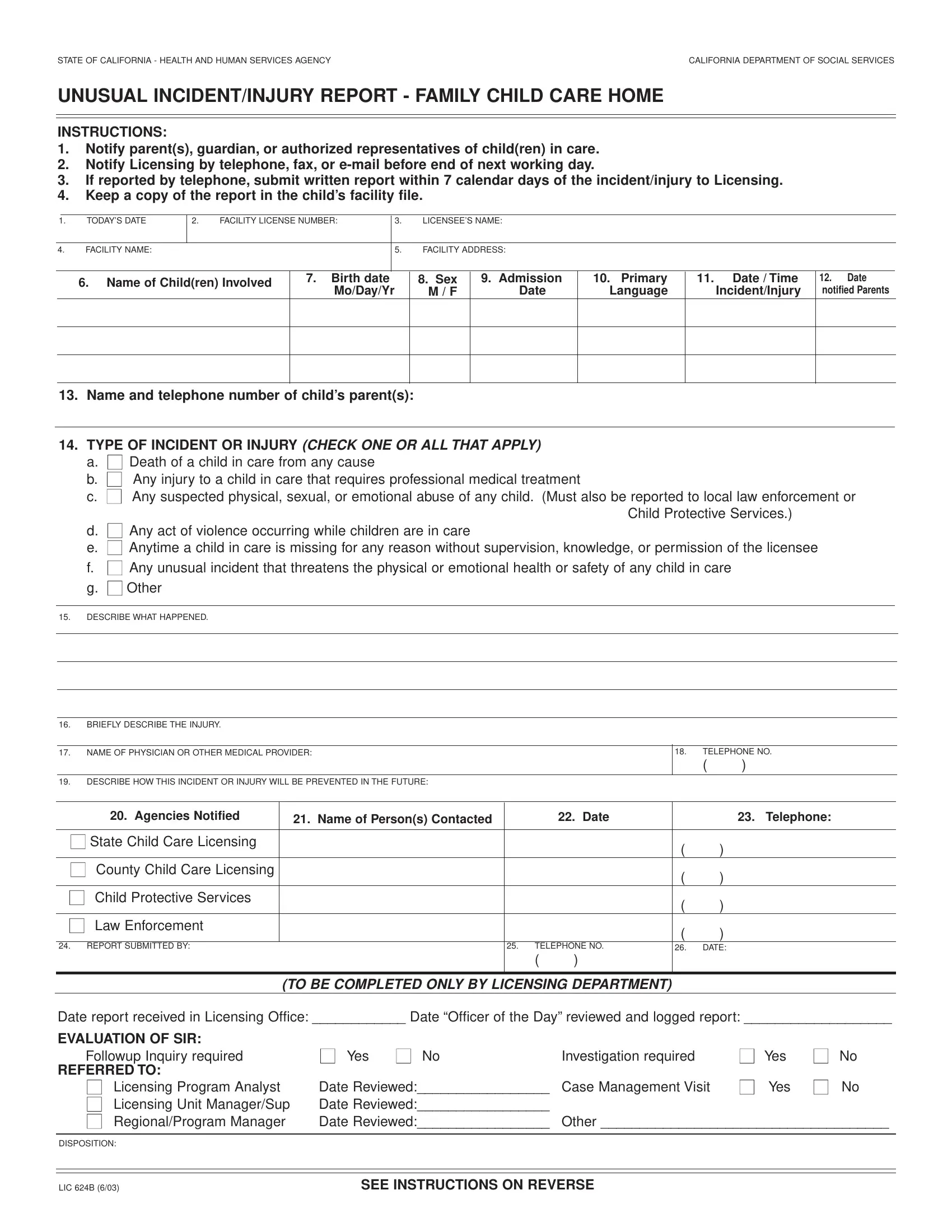
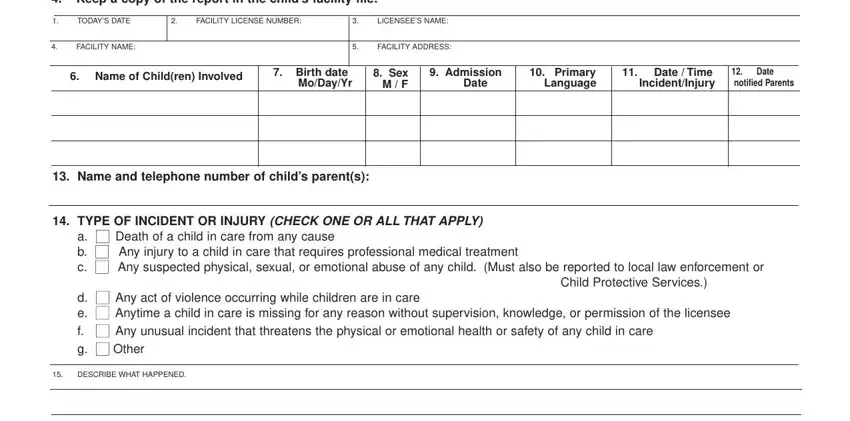
UNUSUAL INCIDENT/INJURY REPORT - FAMILY CHILD CARE HOME
INSTRUCTIONS:
1.Notify parent(s), guardian, or authorized representatives of child(ren) in care.
2.Notify Licensing by telephone, fax, or e-mail before end of next working day.
3.If reported by telephone, submit written report within 7 calendar days of the incident/injury to Licensing.
4.Keep a copy of the report in the child’s facility file.
2.FACILITY LICENSE NUMBER:
6.Name of Child(ren) Involved
11.Date / Time Incident/Injury
13.Name and telephone number of child’s parent(s):
14.TYPE OF INCIDENT OR INJURY (CHECK ONE OR ALL THAT APPLY)
a.■ Death of a child in care from any cause
b.■ Any injury to a child in care that requires professional medical treatment
c.■ Any suspected physical, sexual, or emotional abuse of any child. (Must also be reported to local law enforcement or Child Protective Services.)
d.■ Any act of violence occurring while children are in care
e.■ Anytime a child in care is missing for any reason without supervision, knowledge, or permission of the licensee
f.■ Any unusual incident that threatens the physical or emotional health or safety of any child in care
g.■ Other
15.DESCRIBE WHAT HAPPENED.
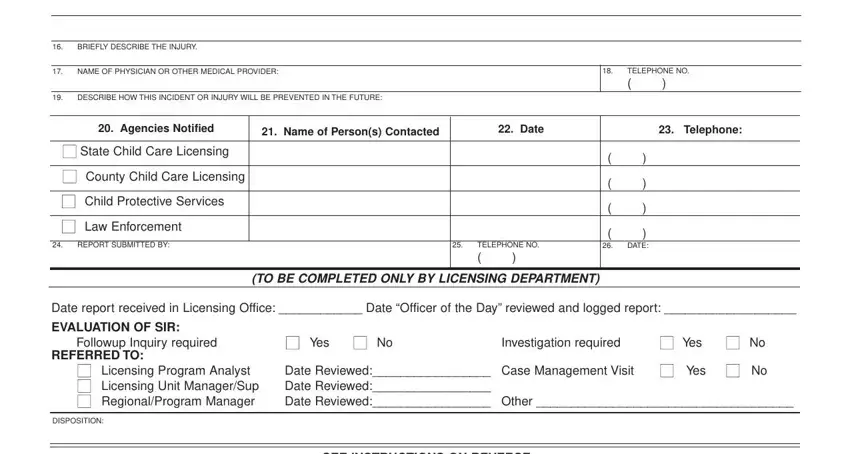
16.BRIEFLY DESCRIBE THE INJURY.
17.NAME OF PHYSICIAN OR OTHER MEDICAL PROVIDER:
19.DESCRIBE HOW THIS INCIDENT OR INJURY WILL BE PREVENTED IN THE FUTURE:
20. Agencies Notified |
21. Name of Person(s) Contacted |
|
|
22. Date |
|
23. Telephone: |
|
|
|
|
|
|
|
■ State Child Care Licensing |
|
|
|
|
( |
) |
|
|
|
|
|
■ County Child Care Licensing |
|
|
|
|
( |
) |
|
|
|
|
|
■ Child Protective Services |
|
|
|
|
( |
) |
|
|
|
|
|
■ Law Enforcement |
|
|
|
|
( |
) |
|
|
|
|
|
24. REPORT SUBMITTED BY: |
|
25. |
TELEPHONE NO. |
26. |
DATE: |
|
|
|
( |
) |
|
|
|
|
|
|
|
|
|
(TO BE COMPLETED ONLY BY LICENSING DEPARTMENT)
Date report received in Licensing Office: ____________ Date “Officer of the Day” reviewed and logged report: ___________________
EVALUATION OF SIR: |
■ Yes ■ No |
|
■ Yes |
■ No |
Followup Inquiry required |
Investigation required |
REFERRED TO: |
|
|
|
|
■ Licensing Program Analyst |
Date Reviewed:_________________ |
Case Management Visit |
■ Yes |
■ No |
■ Licensing Unit Manager/Sup |
Date Reviewed:_________________ |
|
|
|
■ Regional/Program Manager |
Date Reviewed:_________________ |
Other _____________________________________ |
DISPOSITION:
SEE INSTRUCTIONS ON REVERSE
GENERAL INSTRUCTIONS FOR COMPLETION
1.Enter the current month, day, and year.
2.Enter the facility number as shown on the license.
3.Enter the licensee’s name as shown on license.
4.Enter the name of the facility as shown on the license.
5.Enter the number and street address, city, state, and zip code.
6.Enter the first and last name of each child involved in the incident or injury.
7.Enter the month, date, and year of the child’s birth date.
8.Enter the gender of the child as M for Male or F for Female.
9.Enter the month, date, and year the child was accepted into the Family Child Care Home.
10.Enter the language that the child speaks(i.e., English, Spanish, etc.).
11.Enter the month, date, year and the time of day that the incident or injury happened.
12.Enter the month, date, and year that the child’s parent(s) were notified.
13.Enter the name(s) and telephone number of the child’s parent(s).
14.Type of Incident or injury definitions:
a.Check if a child in care has died from any cause.
b.Check if a child was injured while in care, and the injury required professional medical treatment other than first aid.
c.Check if it is suspected that a child has been subjected to physical, sexual, or emotional abuse.
d.Check if any act of violence occurred while children are in care, whether or not a child was involved.
e.Check if a child in care leaves or wanders (is missing) from the facility without permission or supervision, including when a child is missing during any outing or special event away from the facility, or a child doesn’t return from school.
f.Check if an unusual incident occurs that is not covered above, and threatens the physical or emotional health or safety of a child in care. This category may include epidemic outbreaks, poisonings, fires, or other catastrophes.
g.Check other if the unusual incident is not covered above.
15.Describe what happened. Be specific. Include name of person(s) involved in or suspected of causing the injury.
16.Describe the injury.
17.Enter the first and last name and title of the doctor providing care to child, if known.
18.Enter the area code and seven digit telephone number of the doctor or hospital where care was given.
19.Describe how this incident or injury will be prevented in the future.
20.Check one or more of the agencies notified of the incident or injury.
21.Enter the name of the person (for each agency) with whom you spoke when reporting the injury.
22.Enter the month, day, and year next to the agency person’s name that was contacted.
23.Enter the area code and seven digit telephone number of the agency contacted.
24.Enter the first and last name and title of the person filling out this report.
25.Enter the area code and seven digit telephone number of the person filling out this report.
26.Enter the month, date, and year this report was filled out.