
When working in the online PDF editor by FormsPal, you are able to complete or change kentucky chfs 529 information right here. In order to make our editor better and more convenient to utilize, we consistently develop new features, with our users' suggestions in mind. With just a couple of simple steps, you can begin your PDF editing:
Step 1: First of all, open the pdf editor by pressing the "Get Form Button" above on this site.
Step 2: This tool enables you to work with the majority of PDF files in a variety of ways. Change it by writing personalized text, correct what is originally in the PDF, and include a signature - all when you need it!
Filling out this form needs focus on details. Make certain every blank field is completed accurately.
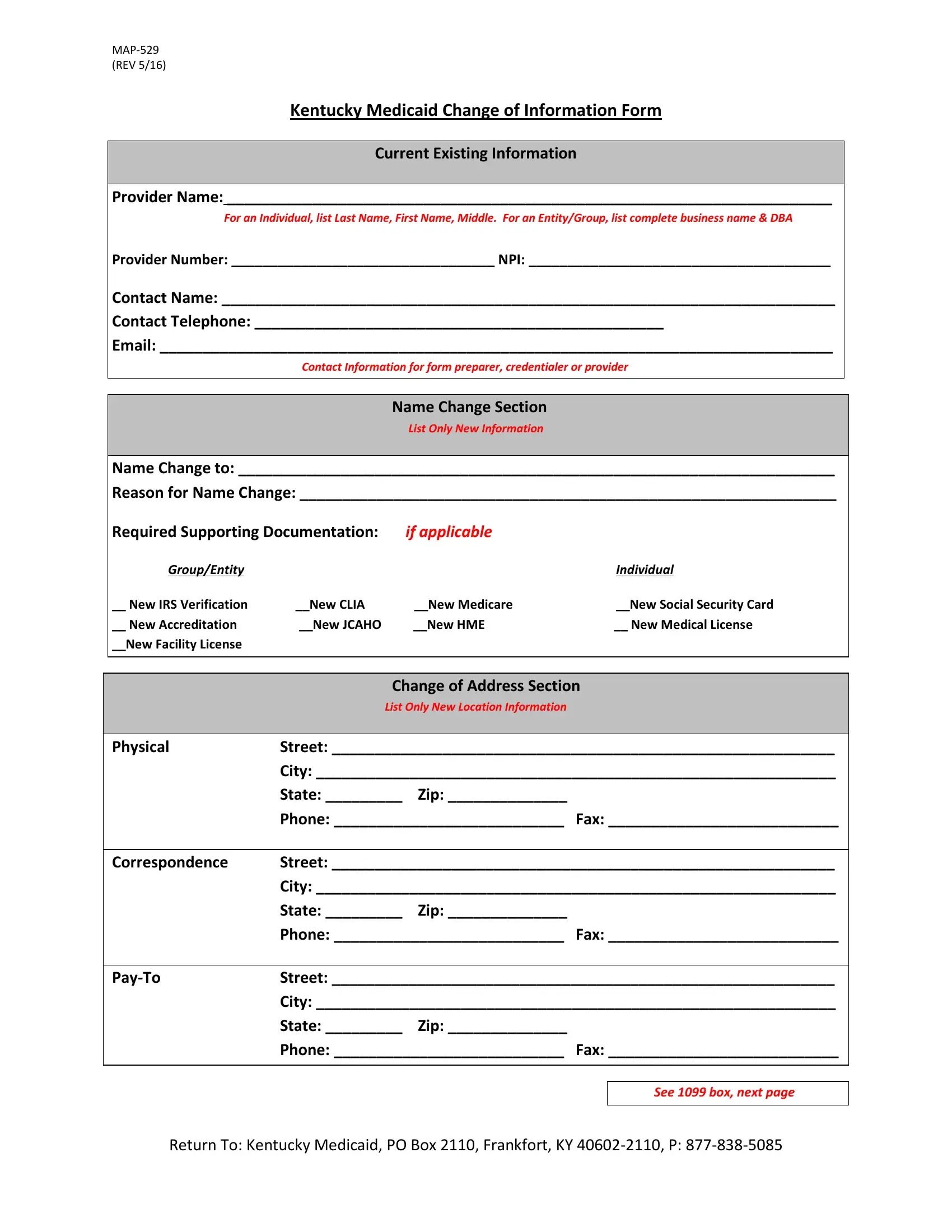
1. It is critical to complete the kentucky chfs 529 information accurately, so pay close attention while working with the segments that contain all these blanks:
2. Once your current task is complete, take the next step – fill out all of these fields - New Accreditation, New JCAHO New HME, New Medical License, New Facility License, Change of Address Section, List Only New Location Information, Physical, Street, City, State Zip, Phone Fax, Correspondence, Street, City, and State Zip with their corresponding information. Make sure to double check that everything has been entered correctly before continuing!
You can easily make errors when filling out the City, hence be sure you take another look before you decide to send it in.
3. In this specific part, check out Street, City, State Zip, Phone Fax, Additional Location Section, List Only New Location Information, Physical Address, Street, City, State Zip, Phone Fax, Physical Address, Street, City, and State Zip. Each of these have to be filled out with greatest precision.
4. To move onward, this form section requires typing in several fields. Examples include Contact Name, Contact Telephone, Email, Contact Information for form, Request To Terminate Kentucky, I request to terminate my, Name, Kentucky Medicaid effective, End Date, Medicaid Number that I am, I authorize Kentucky Medicaid to, on this form For an individual the, and Printed Name Title, which you'll find integral to moving forward with this particular PDF.
Step 3: Before obtaining the next stage, it's a good idea to ensure that blank fields were filled out right. The moment you are satisfied with it, click on “Done." Create a 7-day free trial option with us and gain direct access to kentucky chfs 529 information - download, email, or change from your personal cabinet. FormsPal is focused on the privacy of our users; we always make sure that all information coming through our system is secure.