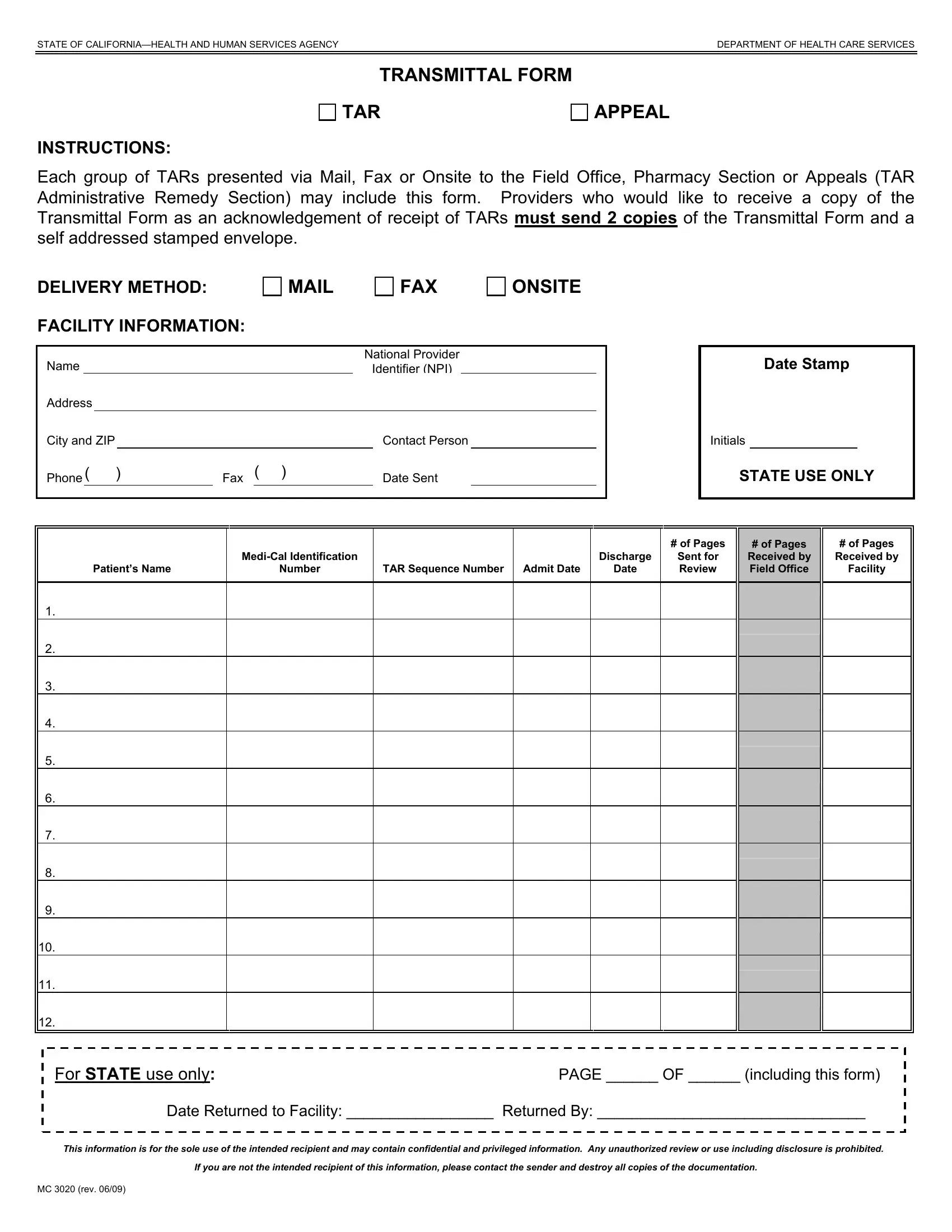
When navigating the complexities of health and healthcare services within California, the MC 3020 form emerges as an essential document for healthcare providers engaging with the state's Health and Human Services Agency, specifically within the Department of Health Care Services. This form, serving as a Transmittal Form for TAR (Treatment Authorization Request) Appeals, represents a crucial step for healthcare providers seeking reconsideration or appeal of decisions related to patient treatment authorizations. The procedure outlined requires the submission of this form whether through mail, fax, or onsite delivery to the appropriate Field Office, Pharmacy Section, or Appeals (TAR Administrative Remedy Section), facilitating a structured approach towards appealing TAR decisions. To ensure acknowledgment of receipt, providers are instructed to send two copies of the form alongside a self-addressed stamped envelope. The form itself captures critical details such as the facility information, including the provider's name, National Provider Identifier (NPI), and contact details, alongside the patient's specific Medi-Cal identification, the pertinent TAR sequence numbers, and dates relevant to the patient's care trajectory. This structured process underscores the commitment of the Department of Health Care Services to streamline appeals while maintaining the integrity and confidentiality of patient information, as indicated by the stringent guidelines governing the handling and destruction of the documentation.
| Question | Answer |
|---|---|
| Form Name | Form Mc 3020 |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | medi, TARs, california, TRANSMITTAL |
STATE OF |
DEPARTMENT OF HEALTH CARE SERVICES |
|
|
|
|
TRANSMITTAL FORM
TAR
APPEAL
INSTRUCTIONS:
Each group of TARs presented via Mail, Fax or Onsite to the Field Office, Pharmacy Section or Appeals (TAR Administrative Remedy Section) may include this form. Providers who would like to receive a copy of the Transmittal Form as an acknowledgement of receipt of TARs must send 2 copies of the Transmittal Form and a self addressed stamped envelope.
DELIVERY METHOD: |
|
|
|
FAX |
ONSITE |
||||||
FACILITY INFORMATION: |
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
Name |
|
|
|
|
National Provider |
|
|
||||
|
|
|
Identifier (NPI) |
|
|
|
|||||
Address |
|
|
|
|
|
|
|
|
|
||
City and ZIP |
|
|
|
|
|
Contact Person |
|
|
|||
Phone ( ) |
Fax ( |
) |
|
Date Sent |
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
Date Stamp
Initials
STATE USE ONLY
|
|
|
|
# of Pages |
|
|
Discharge |
Sent for |
|
Patient’s Name |
Number |
TAR Sequence Number Admit Date |
Date |
Review |
1.
2.
3.
4.
5.
6.
7.
8.
9.
10.
11.
12.
|
# of Pages |
# of Pages |
|
Received by |
Received by |
|
Field Office |
Facility |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
For STATE use only:PAGE ______ OF ______ (including this form)
Date Returned to Facility: _________________ Returned By: _______________________________
This information is for the sole use of the intended recipient and may contain confidential and privileged information. Any unauthorized review or use including disclosure is prohibited.
If you are not the intended recipient of this information, please contact the sender and destroy all copies of the documentation.
MC 3020 (rev. 06/09)