
Using the online PDF editor by FormsPal, you're able to complete or edit inter county transfer medi cal here and now. The tool is continually upgraded by us, receiving cool functions and turning out to be greater. For anyone who is seeking to get going, here's what it will require:
Step 1: First of all, access the tool by clicking the "Get Form Button" above on this webpage.
Step 2: Once you launch the tool, you'll see the form all set to be completed. Other than filling in different blank fields, you can also do some other things with the file, specifically putting on your own words, editing the original text, inserting illustrations or photos, placing your signature to the form, and more.
To be able to complete this form, be sure you type in the right information in each and every blank field:
1. Start completing your inter county transfer medi cal with a group of necessary blanks. Collect all of the important information and be sure there is nothing overlooked!
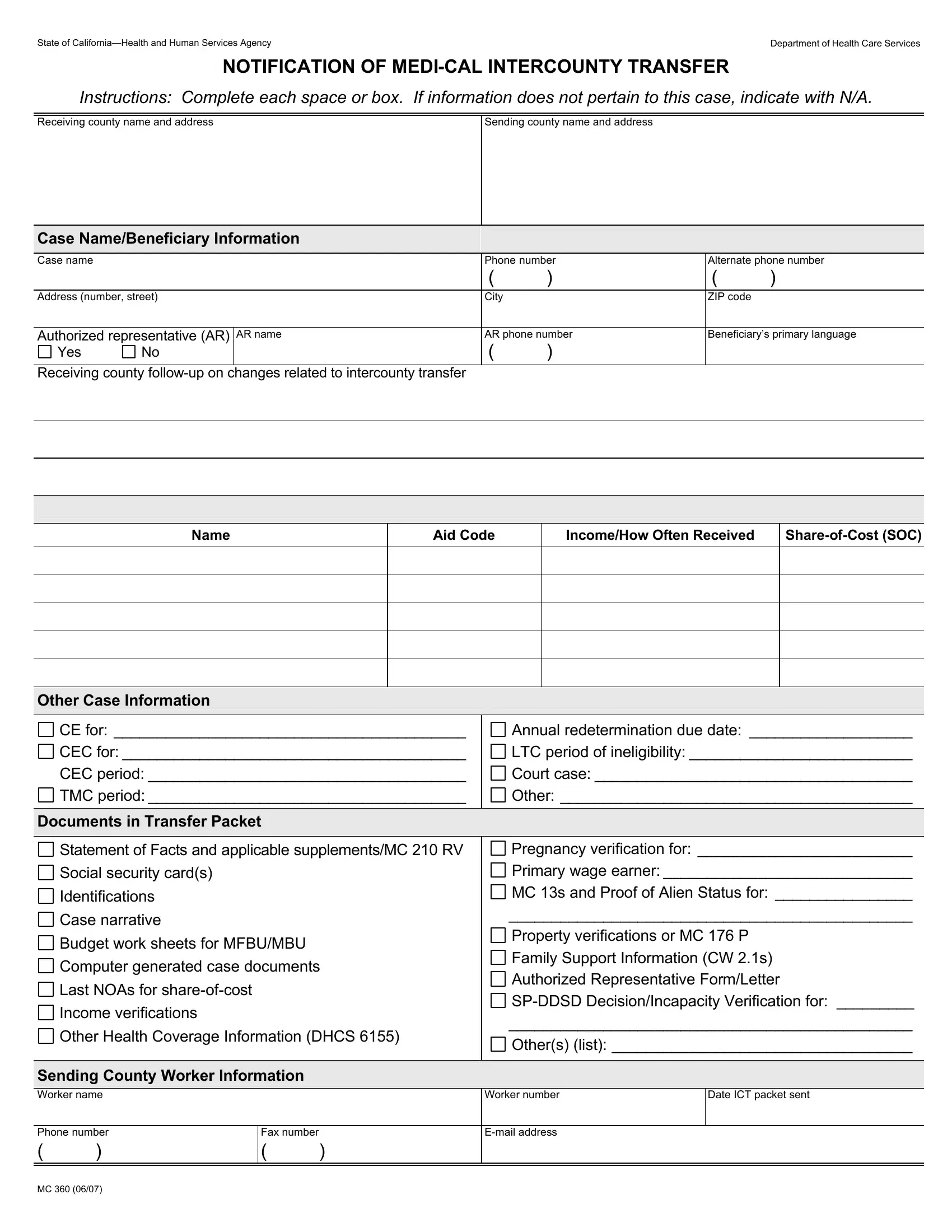
2. When this selection of blank fields is completed, proceed to enter the suitable details in these: Name, Aid Code, IncomeHow Often Received, ShareofCost SOC, Other Case Information, CE for CEC for CEC period TMC, Annual redetermination due date, Documents in Transfer Packet, Statement of Facts and applicable, Social security cards, Identifications, Case narrative, Budget work sheets for MFBUMBU, Computer generated case documents, and Last NOAs for shareofcost.
3. Completing Other Health Coverage Information, Sending County Worker Information, Pregnancy verification for, Worker number, Date ICT packet sent, Phone number, Fax number, and Email address is essential for the next step, make sure to fill them out in their entirety. Don't miss any details!
In terms of Sending County Worker Information and Pregnancy verification for, ensure that you double-check them in this section. Those two are the most significant ones in the form.
Step 3: After you have glanced through the details you given, click "Done" to conclude your FormsPal process. Right after creating a7-day free trial account here, you'll be able to download inter county transfer medi cal or send it through email without delay. The PDF form will also be accessible via your personal account with all of your adjustments. We do not share or sell any details that you type in while working with documents at our website.