
 Determination pending
Determination pending 
 Return to medical exam office for
Return to medical exam office for 
 Medical Examination Report amended
Medical Examination Report amended 
 Other Practitioner
Other Practitioner 
 Does not meet standards in
Does not meet standards in  Meets standards in
Meets standards in  Meets standards, but periodic monitoring required
Meets standards, but periodic monitoring required 
 Other Practitioner
Other Practitioner We were building our PDF editor having the concept of making it as quick make use of as possible. For this reason the actual procedure of filling out the medical exam form is going to be smooth carry out the following steps:
Step 1: On this website page, choose the orange "Get form now" button.
Step 2: Now you are able to manage medical exam form. You've got lots of options thanks to our multifunctional toolbar - you'll be able to add, erase, or alter the information, highlight its specified elements, as well as carry out many other commands.
These segments are going to make up your PDF document:
Type in the appropriate information in the space Are you currently taking, Yes, No Not Sure, and This document contains sensitive.
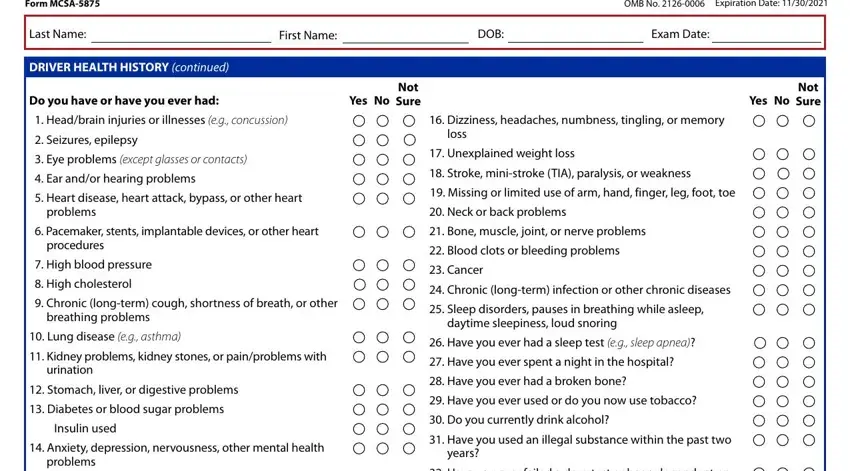
The program will request you to insert certain vital data to automatically fill out the field Form MCSA, Last Name, First Name, DOB, Exam Date, OMB No, Expiration Date, DRIVER HEALTH HISTORY continued, Do you have or have you ever had, Yes No, Not Sure, Yes No, Not Sure, Headbrain injuries or illnesses, and Dizziness headaches numbness.
The Fainting or passing out, Have you ever failed a drug test, an illegal substance, Other health conditions not, Yes, Not Sure, Did you answer yes to any of, Yes, Not Sure, CMV DRIVERS SIGNATURE, I certify that the above, Drivers Signature, and Date box will be your place to put the rights and obligations of all parties.
Finish by looking at the following sections and filling them in as required: Review and discuss pertinent, and Page.

Step 3: Choose the "Done" button. Now it's possible to export the PDF file to your device. Aside from that, it is possible to forward it via electronic mail.
Step 4: It is easier to have duplicates of the document. You can rest assured that we will not publish or check out your data.
