In order to ensure that your business is in compliance with the current tax code, it's important to file Form Mfut 12. This form is used to calculate the amount of withholding tax that should be deducted from each employee's wages. By filing this form, you can be sure that your employees are being taxed correctly and that you're in compliance with the law. If you need help filling out this form, or if you have any other questions about tax withholdings, please contact a professional accountant or tax specialist. Thank you for your time.
| Question | Answer |
|---|---|
| Form Name | Form Mfut 12 |
| Form Length | 2 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 30 sec |
| Other names | 2003 MFUT-12 Application for Motor Fuel Use Tax IFTA License and Decals. Motor Fuel Use |
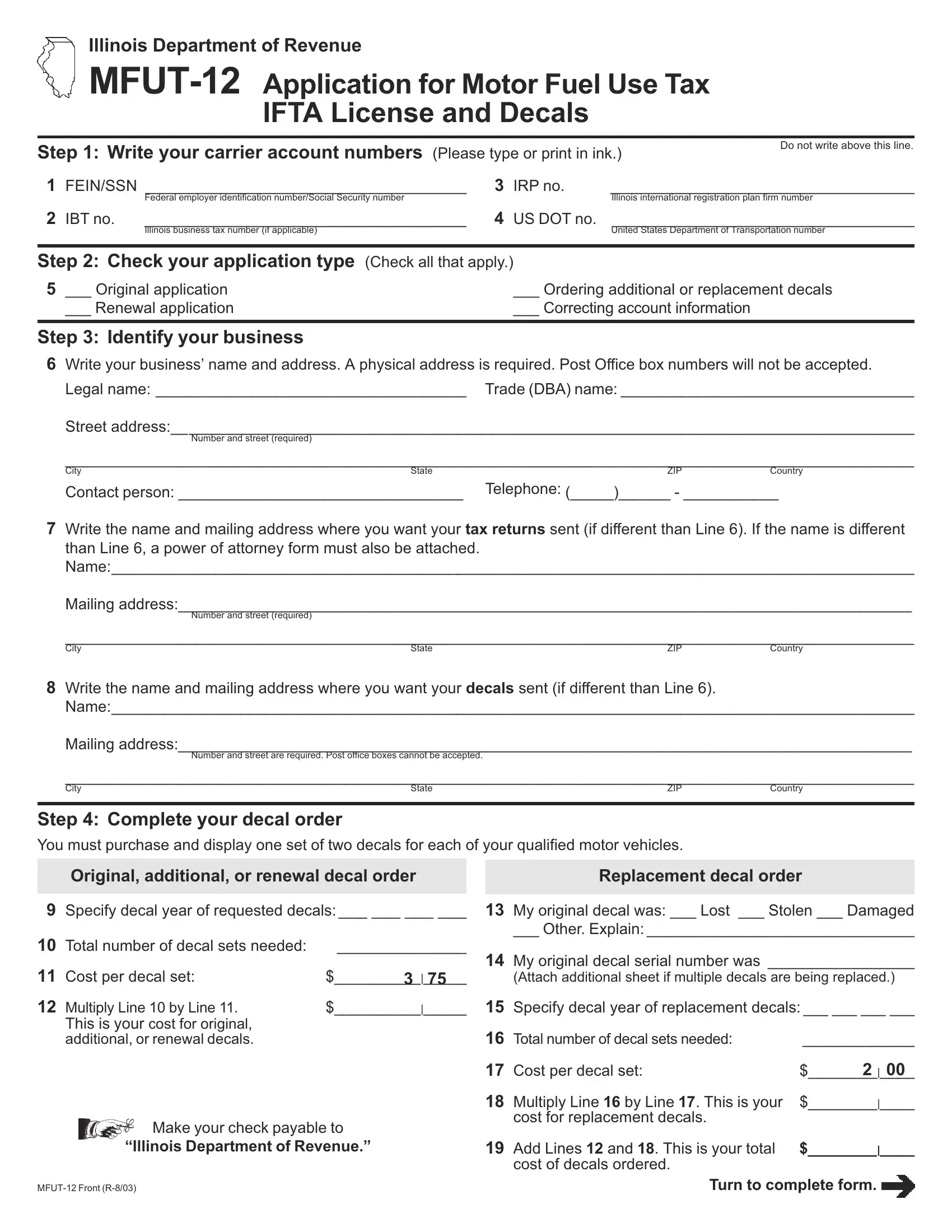
Illinois Department of Revenue
IFTA License and Decals
Step 1: Write your carrier account numbers (Please type or print in ink.)
Do not write above this line.
1 |
FEIN/SSN _____________________________________ |
3 |
IRP no. |
___________________________________ |
|
|
|
Federal employer identification number/Social Security number |
|
|
Illinois international registration plan firm number |
2 |
IBTno. |
_____________________________________ |
4 |
US DOT no. |
___________________________________ |
|
|
Illinois business tax number (if applicable) |
|
|
United States Department of Transportation number |
Step 2: Check your application type (Check all that apply.)
5 ___ Original application |
___ Ordering additional or replacement decals |
___ Renewal application |
___ Correcting account information |
|
|
Step 3: Identifyyourbusiness
6Write your business’ name and address. A physical address is required. Post Office box numbers will not be accepted.
Legal name: ____________________________________ Trade(DBA)name:__________________________________
Street address:______________________________________________________________________________________
Number and street (required)
_________________________________________________________________________________________________
City |
State |
ZIP |
Country |
Contact person: _________________________________ |
Telephone: (_____)______ - ___________ |
||
7Write the name and mailing address where you want your tax returns sent (if different than Line 6). If the name is different than Line 6, a power of attorney form must also be attached. Name:_____________________________________________________________________________________________
Mailing address:_____________________________________________________________________________________
Number and street (required)
_________________________________________________________________________________________________
City |
State |
ZIP |
Country |
8Write the name and mailing address where you want your decals sent (if different than Line 6).
Name:_____________________________________________________________________________________________
Mailing address:_____________________________________________________________________________________
Number and street are required. Post office boxes cannot be accepted.
_________________________________________________________________________________________________
City |
State |
ZIP |
Country |
Step 4: Complete your decal order
You must purchase and display one set of two decals for each of your qualified motor vehicles.
Original, additional, or renewal decal order
9Specify decal year of requested decals:___ ___ ___ ___
10 |
Total number of decal sets needed: |
|
_______________ |
11 |
Cost per decal set: |
$ |
3 | 75 |
12 |
Multiply Line 10 by Line 11. |
$ |
__________|_____ |
|
This is your cost for original, |
|
|
|
additional,orrenewaldecals. |
|
|
Make your check payable to
“IllinoisDepartmentofRevenue.”
Replacement decal order
13My original decal was: ___ Lost ___ Stolen ___ Damaged
___ Other. Explain:_______________________________
14My original decal serial number was _________________
(Attach additional sheet if multiple decals are being replaced.)
15Specify decal year of replacement decals:___ ___ ___ ___
16 |
Totalnumberofdecalsetsneeded: |
_____________ |
|
17 |
Cost per decal set: |
$ |
2 | 00 |
18 |
Multiply Line 16 by Line 17. This is your |
$ |
________|____ |
|
cost for replacement decals. |
|
|
19 |
Add Lines 12 and 18. This is your total |
$________|____ |
|
|
cost of decals ordered. |
|
|
Turn to complete form.
Step 5: Identify your type of operation
20 |
Check your type of business ownership. |
|
|
|
|
____ Individual ____ Corporation ____ Partnership ____ State/federal government |
____ |
||
21 |
If you checked “Corporation,” write the date and state of incorporation. |
__ __/__ __/__ __ __ __ |
______________ |
|
|
|
Month Day |
Year |
State |
22List the owners or corporate officers.
SocialSecurityno. |
Name and title |
City and state |
__ _ - _ _ - _ _ _ _ __________________________________________________ _______________________________
__ _ - _ _ - _ _ _ _ __________________________________________________ _______________________________
__ _ - _ _ - _ _ _ _ __________________________________________________ _______________________________
__ _ - _ _ - _ _ _ _ __________________________________________________ _______________________________
23 Do you currently have or have you ever had an IFTA license from a state other than Illinois? ____ yes ____ no
If you checked “yes,” tell us in what jurisdictions you were previously licensed. ____________________________________
Step 6: Tell us your fuel types, operations, and bulk fuel storage
24List the number of qualified motor vehicles you own or operate interstate________________________________________
25List the number of qualified motor vehicles you own or operate intrastate________________________________________
26Check the type of fuels used in the qualified motor vehicles you own or operate:
❒ |
Diesel |
❒ |
Gasoline |
❒ |
Gasohol |
❒ |
LP gas |
❒ |
Compressed natural gas |
❒ |
Ethanol |
❒ |
Methanol |
❒ |
❒ |
❒ |
27List each jurisdiction in which you maintain bulk fuel storage. Attach additional sheets if necessary.
______________________ |
________________________ |
________________________ |
_______________________ |
______________________ |
________________________ |
________________________ |
_______________________ |
______________________ |
________________________ |
________________________ |
_______________________ |
______________________ |
________________________ |
________________________ |
_______________________ |
______________________ |
________________________ |
________________________ |
_______________________ |
______________________ |
________________________ |
________________________ |
_______________________ |
______________________ |
________________________ |
________________________ |
_______________________ |
______________________ |
________________________ |
________________________ |
_______________________ |
Step 7: Signbelow
Your FEIN or SSN is used for account identification, payment processing, and record keeping. Your number and pertinent account information may be provided to IFTA jurisdictions, governmental and state agencies, and any persons necessary for administering the Motor Fuel Tax Law.
Underpenaltiesofperjury,IstatethatIhaveexaminedthisapplicationand,tothebestofmyknowledge,itistrue,correct,andcomplete.Theapplicant agreestocomplywithalllicensedisplay,recordkeeping,reporting,andpaymentrequirementsasspecifiedintheIllinoisMotorFuelTaxLawandthe InternationalFuelTaxAgreement.ApplicantfurtheragreesthattheIllinoisDepartmentofRevenuemaywithholdanyoverpaymentsdueifitisdelinquent onpaymentsofmotorfuelusetaxesduethestateofIllinoisoranyIFTAmemberjurisdiction.Applicantunderstandsthatfailuretocomplywiththese provisionsisgroundsforrevocationofitslicenseinallapplicablejurisdictions.
Note: Without proper signature from an owner, partner, authorized corporate officer, authorized agent, or employee who has the control, supervision, or responsibility of filing returns and making payment of the tax, your application will be denied.
_________________________________________________ |
Mail to: |
MOTORFUELUSETAXSECTION |
||
|
ILLINOIS DEPARTMENT OF REVENUE |
|||
Signature |
|
|
|
|
_______________________ |
|
|
|
POBOX19467 |
|
|
|
SPRINGFIELD IL |
|
Title |
|
|
|
|
|
|
|
|
|
(_____) _____ - _________ |
__ __/__ __/__ __ __ __ |
|
Telephone: 217 |
|
Telephone |
Month Day |
Year |
|
|
This form is authorized by the Illinois Motor Fuel Tax Law. Disclosure of this information is REQUIRED. Failure to provide information could result in a penalty. This form has been approved by the Forms Management Center.