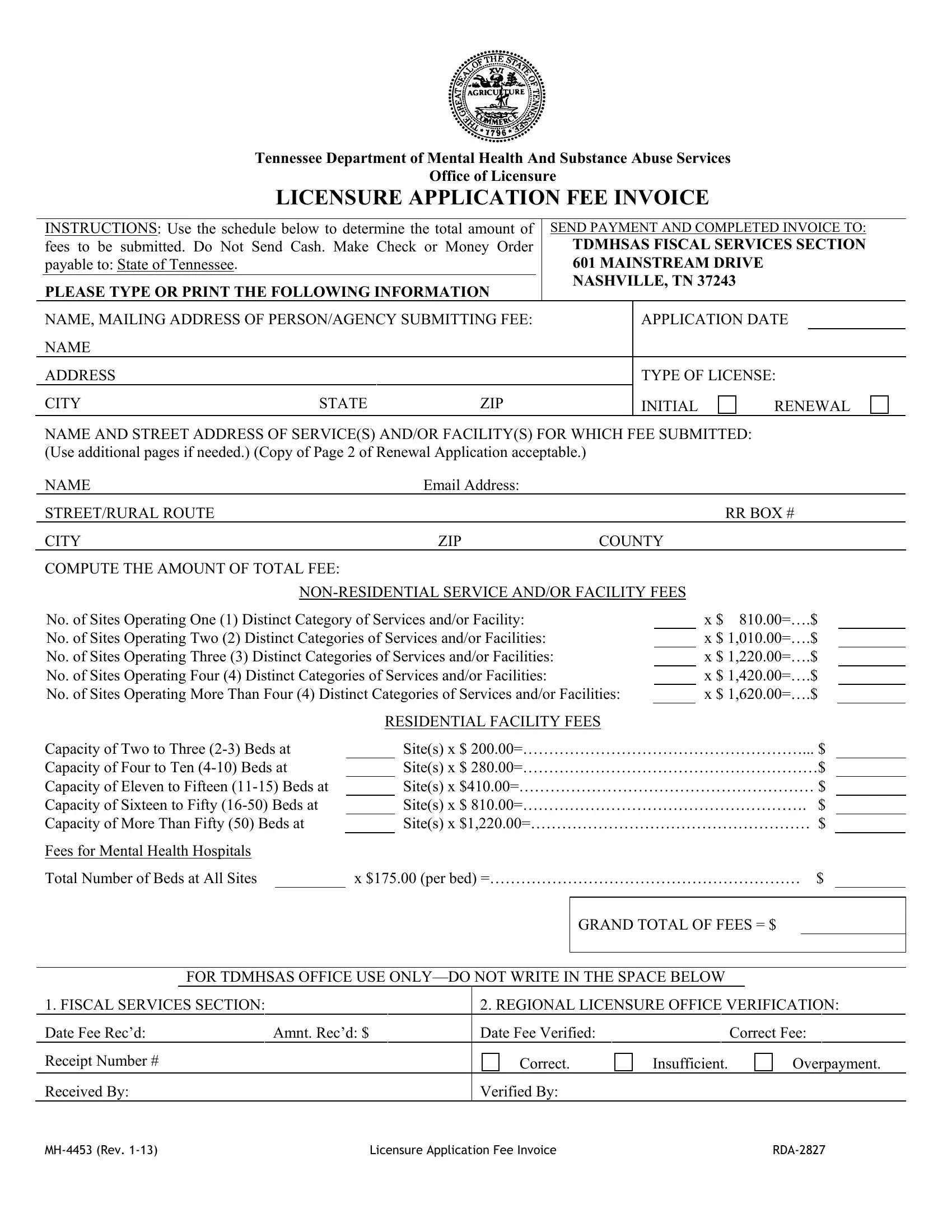
The MH 4453 form serves a critical role within the legislative and operational framework established by the Tennessee Department of Mental Health and Substance Abuse Services Office of Licensure. As an explicit mechanism designed to regulate the financial transactions associated with licensure applications, this document facilitates a structured procedure for entities seeking authorization or renewal for providing mental health and substance abuse services. This reliance on a predetermined schedule to compute total fees underscores the state's commitment to transparency and accountability in its financial dealings. Entities are required not only to furnish comprehensive contact information but also to detail the specifics of the services and/or facilities for which licensure is sought, thereby aligning operational scope with fiscal responsibilities. The form meticulously categorizes fees based on service types, ranging from non-residential to residential facilities, and further tailors the fee structure to accommodate the varying capacities of these facilities. This tiered approach to fee assessment, coupled with explicit instructions for payment submission, exemplifies the meticulous planning and organization the state upholds to ensure a seamless licensure process. Furthermore, the form's provision for office use only adds an additional layer of scrutiny, ensuring that all financial transactions are accurately recorded and verified, reinforcing the system's integrity and the equitable treatment of all applicants.
| Question | Answer |
|---|---|
| Form Name | Form Mh 4453 |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | ApplicFeesInv tdmh fiscal services form |
Tennessee Department of Mental Health And Substance Abuse Services
Office of Licensure
LICENSURE APPLICATION FEE INVOICE
|
INSTRUCTIONS: Use the schedule below to determine the total amount of |
|
SEND PAYMENT AND COMPLETED INVOICE TO: |
|||||
|
fees to be submitted. Do Not Send Cash. Make Check or Money Order |
|
TDMHSAS FISCAL SERVICES SECTION |
|||||
|
payable to: State of Tennessee. |
|
|
|
601 MAINSTREAM DRIVE |
|
|
|
|
PLEASE TYPE OR PRINT THE FOLLOWING INFORMATION |
|
NASHVILLE, TN 37243 |
|
|
|||
|
|
|
|
|
|
|||
|
NAME, MAILING ADDRESS OF PERSON/AGENCY SUBMITTING FEE: |
|
|
APPLICATION DATE |
||||
|
NAME |
|
|
|
|
|
|
|
|
ADDRESS |
|
|
|
|
TYPE OF LICENSE: |
||
|
CITY |
STATE |
ZIP |
|
|
INITIAL |
RENEWAL |
|
NAME AND STREET ADDRESS OF SERVICE(S) AND/OR FACILITY(S) FOR WHICH FEE SUBMITTED: (Use additional pages if needed.) (Copy of Page 2 of Renewal Application acceptable.)
NAME |
Email Address: |
|
STREET/RURAL ROUTE |
|
RR BOX # |
CITY |
ZIP |
COUNTY |
COMPUTE THE AMOUNT OF TOTAL FEE: |
|
|
|
||
No. of Sites Operating One (1) Distinct Category of Services and/or Facility: No. of Sites Operating Two (2) Distinct Categories of Services and/or Facilities: No. of Sites Operating Three (3) Distinct Categories of Services and/or Facilities: No. of Sites Operating Four (4) Distinct Categories of Services and/or Facilities:
No. of Sites Operating More Than Four (4) Distinct Categories of Services and/or Facilities:
x $ |
810.00=….$ |
x $ |
1,010.00=….$ |
x $ |
1,220.00=….$ |
x $ |
1,420.00=….$ |
x $ |
1,620.00=….$ |
Capacity of Two to Three
Fees for Mental Health Hospitals
Total Number of Beds at All Sites
RESIDENTIAL FACILITY FEES
Site(s) x $ 200.00=………………………………………………... $
Site(s) x $ 280.00=…………………………………………………$
Site(s) x $410.00=………………………………………………… $
Site(s) x $ 810.00=………………………………………………. $
Site(s) x $1,220.00=……………………………………………… $
x $175.00 (per bed) =…………………………………………………… $
|
|
|
|
|
GRAND TOTAL OF FEES = $ |
|||
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|||
|
FOR TDMHSAS OFFICE USE |
|
|
|
||||
1. FISCAL SERVICES SECTION: |
|
|
2. REGIONAL LICENSURE OFFICE VERIFICATION: |
|||||
Date Fee Rec’d: |
Amnt. Rec’d: $ |
|
Date Fee Verified: |
Correct Fee: |
||||
Receipt Number # |
|
|
Correct. |
Insufficient. |
|
Overpayment. |
||
Received By: |
|
|
Verified By: |
|
|
|
|
|
|
Licensure Application Fee Invoice |
|
|
|||||