Miosha 300A is a new form that has recently been released by the Social Security Administration. This form is designed to help individuals with their disability claims. The purpose of this blog post is to provide an overview of Form Miosha 300A, and explain how it can be used to support your disability claim. If you are considering filing for disability benefits, it is important to understand how Form Miosha 300A can help you during the application process. We will discuss the basics of this form, and explain why it is important for your claim. Stay tuned for future posts in which we will dive into more detail about how Form Miosha 300A can be used to support your case. Thanks for reading!
| Question | Answer |
|---|---|
| Form Name | Form Miosha 300A |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | R408, miosha form 300a, recordable, ve |
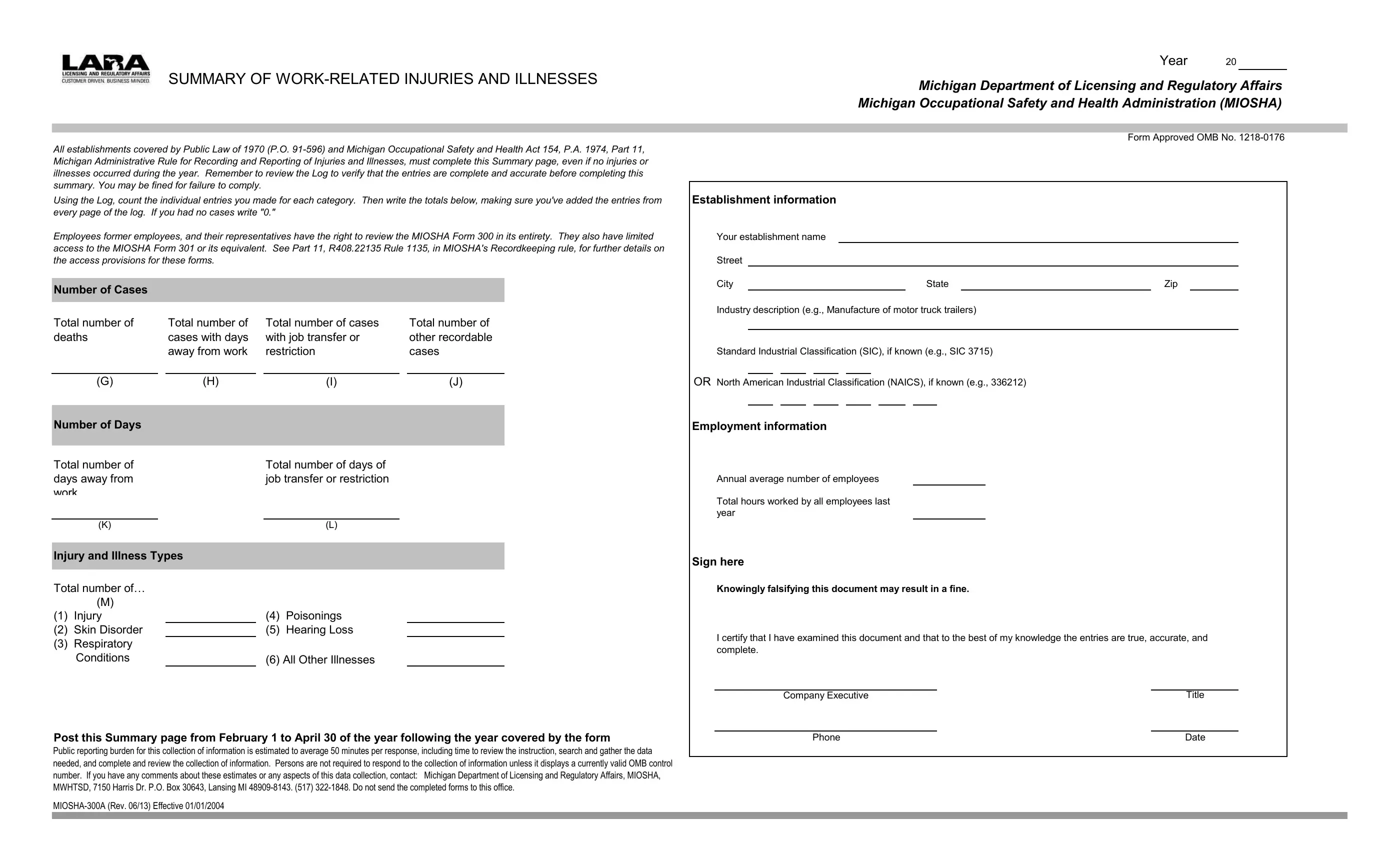
SUMMARY OF
All establishments covered by Public Law of 1970 (P.O.
Using the Log, count the individual entries you made for each category. Then write the totals below, making sure you've added the entries from every page of the log. If you had no cases write "0."
Employees former employees, and their representatives have the right to review the MIOSHA Form 300 in its entirety. They also have limited access to the MIOSHA Form 301 or its equivalent. See Part 11, R408.22135 Rule 1135, in MIOSHA's Recordkeeping rule, for further details on the access provisions for these forms.
Number of Cases |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
Total number of |
|
Total number of |
|
Total number of cases |
|
Total number of |
||
deaths |
|
cases with days |
|
with job transfer or |
|
other recordable |
||
|
|
|
away from work |
|
restriction |
|
cases |
|
|
|
|
|
|
|
|
|
|
|
(G) |
|
(H) |
|
|
(I) |
|
(J) |
|
|
|
|
|
|
|
|
|
Number of Days |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
Total number of |
|
|
|
Total number of days of |
|
|
||
days away from |
|
|
|
job transfer or restriction |
|
|
||
work |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
(K) |
|
|
|
|
(L) |
|
|
|
|
|
|
|
|
|
||
Injury and Illness Types |
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
Total number of… |
|
|
|
|
|
|
|
|
|
(M) |
|
|
|
|
|
|
|
(1) |
Injury |
|
|
(4) |
Poisonings |
|
|
|
(2) |
Skin Disorder |
|
|
(5) |
Hearing Loss |
|
|
|
(3) |
Respiratory |
|
|
|
|
|
|
|
|
Conditions |
|
|
|
(6) All Other Illnesses |
|
|
|
Post this Summary page from February 1 to April 30 of the year following the year covered by the form
Public reporting burden for this collection of information is estimated to average 50 minutes per response, including time to review the instruction, search and gather the data needed, and complete and review the collection of information. Persons are not required to respond to the collection of information unless it displays a currently valid OMB control number. If you have any comments about these estimates or any aspects of this data collection, contact: Michigan Department of Licensing and Regulatory Affairs, MIOSHA, MWHTSD, 7150 Harris Dr. P.O. Box 30643, Lansing MI
Year 20
Michigan Department of Licensing and Regulatory Affairs
Michigan Occupational Safety and Health Administration (MIOSHA)
Form Approved OMB No.
Establishment information
Your establishment name
Street
City |
|
State |
|
Zip |
Industry description (e.g., Manufacture of motor truck trailers)
Standard Industrial Classification (SIC), if known (e.g., SIC 3715)
OR North American Industrial Classification (NAICS), if known (e.g., 336212)
Employment information
Annual average number of employees
Total hours worked by all employees last year
Sign here
Knowingly falsifying this document may result in a fine.
I certify that I have examined this document and that to the best of my knowledge the entries are true, accurate, and complete.
Company Executive |
|
Title |
|
|
|
Phone |
|
Date |