INSTRUCTIONS FOR COMPLETING THE APPLICATION
The Health Insurance Premium Payment (HIPP) Program pays for the cost of health insurance plans when the Department of Social Services decides it would cost less to buy health insurance to cover medical care than to pay for the care only with MO HealthNet funds. To be eligible for the Health Insurance Premium Payment (HIPP) program, some or all of the persons covered under an insurance policy must be eligible for MO HealthNet.
WHO MUST APPLY?
You must apply to the HIPP program if all of the following are true:
You or a member of your household is applying for MO HealthNet or are MO HealthNet-eligible (excluding spend-down)
You or a member of your household is employed or lost employment within the last thirty days, and
The employer or former employer offers group health insurance coverage.
If the Department of Social Services decides the health insurance plan is cost-effective, you must participate in the HIPP Program.
Applicants’, participants’, parents’, guardians’ or caretakers’ MO HealthNet benefits may be denied or canceled if the applicant, participant, parent, guardian or caretaker does not provide information necessary to establish cost effectiveness or does not enroll in a group health insurance plan that the Department determines is cost effective.
WHO CAN CHOOSE TO APPLY?
You can choose to apply to the HIPP program if you or a member of your household is applying for MO HealthNet or are MO HealthNet- eligible (excluding spend-down) and have health insurance available from sources other than employers (personal policies, credit unions, church affiliations, labor unions, memberships in organizations, etc.) If the Department determines the health insurance plan is cost effective, MO HealthNet will pay the premium.
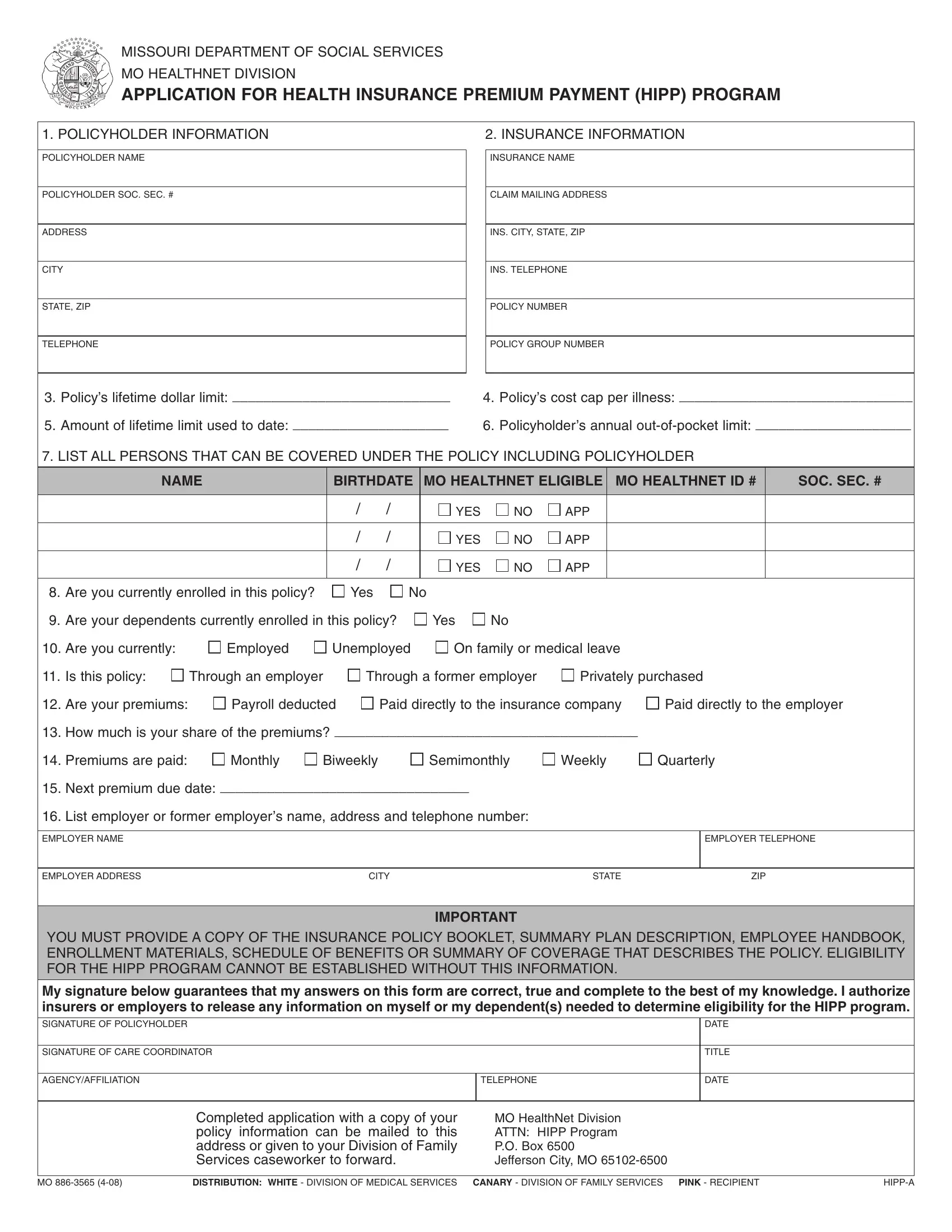
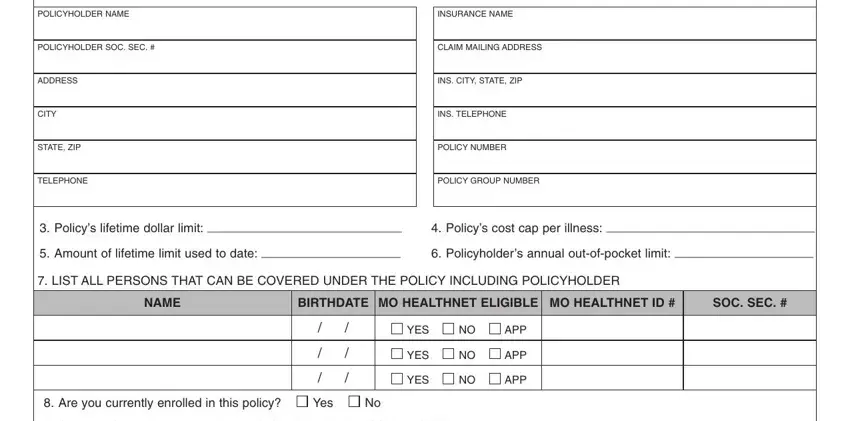
Section 1. List the following information about the policyholder. Name, social security number, address, and telephone number. If you do not have a telephone, list a number where you can be reached or a message left.
Section 2. List the name, claim mailing address and telephone number of the insurance company, the policy number and the policy group number for any insurance you currently have or any insurance offered by your employer or some other source. If your employer or former employer does not offer group health insurance, write “no insurance available” across section 2, then sign and date the application.
Questions Please try to provide as much information as you can obtain regarding the out-of-pocket cost, lifetime limits and caps per illness.
3 - 6.
Section 7. List the name and birth date of everyone in your family who can be covered under this policy, including the policyholder. Check one box (Yes or No) to indicate whether the person is currently on MO HealthNet. If a box is marked yes, write the person’s MO HealthNet identification number (DCN) listed on their MO HealthNet card. If they have applied for MO HealthNet and do not know if they are eligible, the APP (for Applied) box should be checked. List the social security number for each individual.
Question 8. Indicate whether you are currently covered by this insurance policy.
Question 9. Indicate whether your spouse or children are currently covered by this policy.
Question 10. Indicate your current employment status.
Question 11. Indicate if this insurance is through your current employer, a former employer (such as a COBRA plan), or an insurance plan you have purchased on your own.
Question 12. Indicate if your premiums are currently paid through payroll deduction, direct payment to the insurance company or direct payment to the employer.
Question 13. List how much the premium amount is each time a payment is due. If the insurance is through an employer and the employer pays for part of the cost, list only your share of the cost.
Question 14. List how often a premium payment is due. For example: monthly (once a month), biweekly (every two weeks), semimonthly (twice a month), weekly (once a week), quarterly (every three months).
Question 15. List the date your next premium is due.
Section 16. List your employer or former employer’s name, address and telephone number. Employers are contacted to verify payroll deductions, rates, etc.
Signature: Sign and date the application form at the bottom.