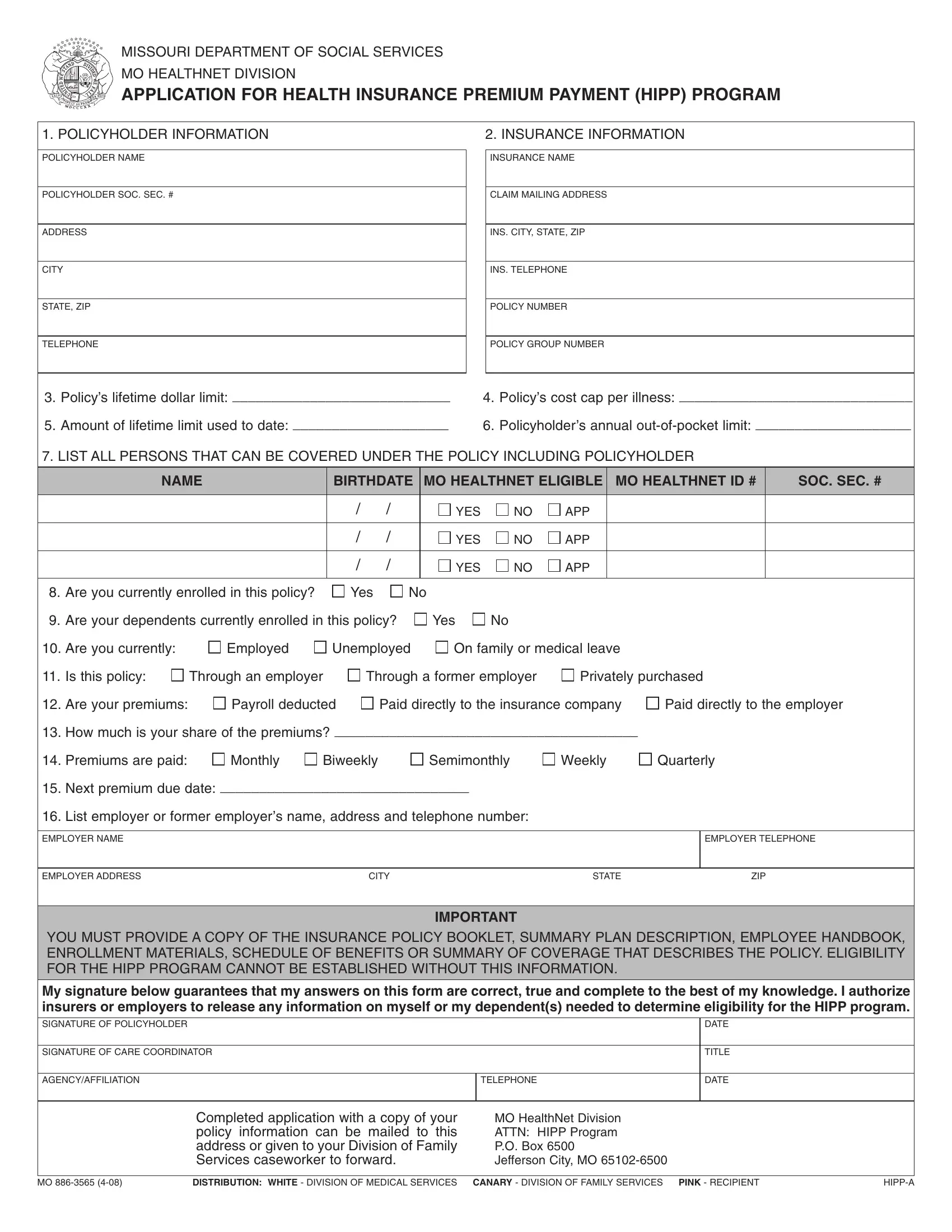
Navigating through the intricacies of health insurance can be daunting, especially when dealing with costs that seem to constantly rise. Enter the MO HealthNet Division's Application for Health Insurance Premium Payment (HIPP) Program, a form designed to provide financial relief to eligible Missouri residents. This comprehensive document, formally known as MO 886 3565, serves as a beacon of hope for policyholders struggling to keep up with their health insurance premiums. By providing detailed information about the policyholder, including social security numbers, addresses, and telephone numbers, along with the specifics of the insurance policy such as insurance name, policy number, and group number, applicants can open the door to potential assistance. The form delves deeper by asking for information about the policy’s lifetime limits, cost caps per illness, and out-of-pocket limits, ensuring a complete understanding of the financial burdens faced. Moreover, it requires listing all family members who could be covered under the policy, their MO HealthNet eligibility, and details regarding the current insurance coverage. Applicants must disclose their employment status, the nature of their policy (whether it’s through an employer, a former employer, or privately purchased), and how premiums are being paid. This detailed application process ensures that those who find themselves overwhelmed by the cost of health insurance have a potential path to reduce their financial load, underscoring the commitment of the Missouri Department of Social Services to support its residents’ healthcare needs.
| Question | Answer |
|---|---|
| Form Name | Form Mo 886 3565 |
| Form Length | 2 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 30 sec |
| Other names | missouri hipp program, caretakers, HEALTHNET, Biweekly |