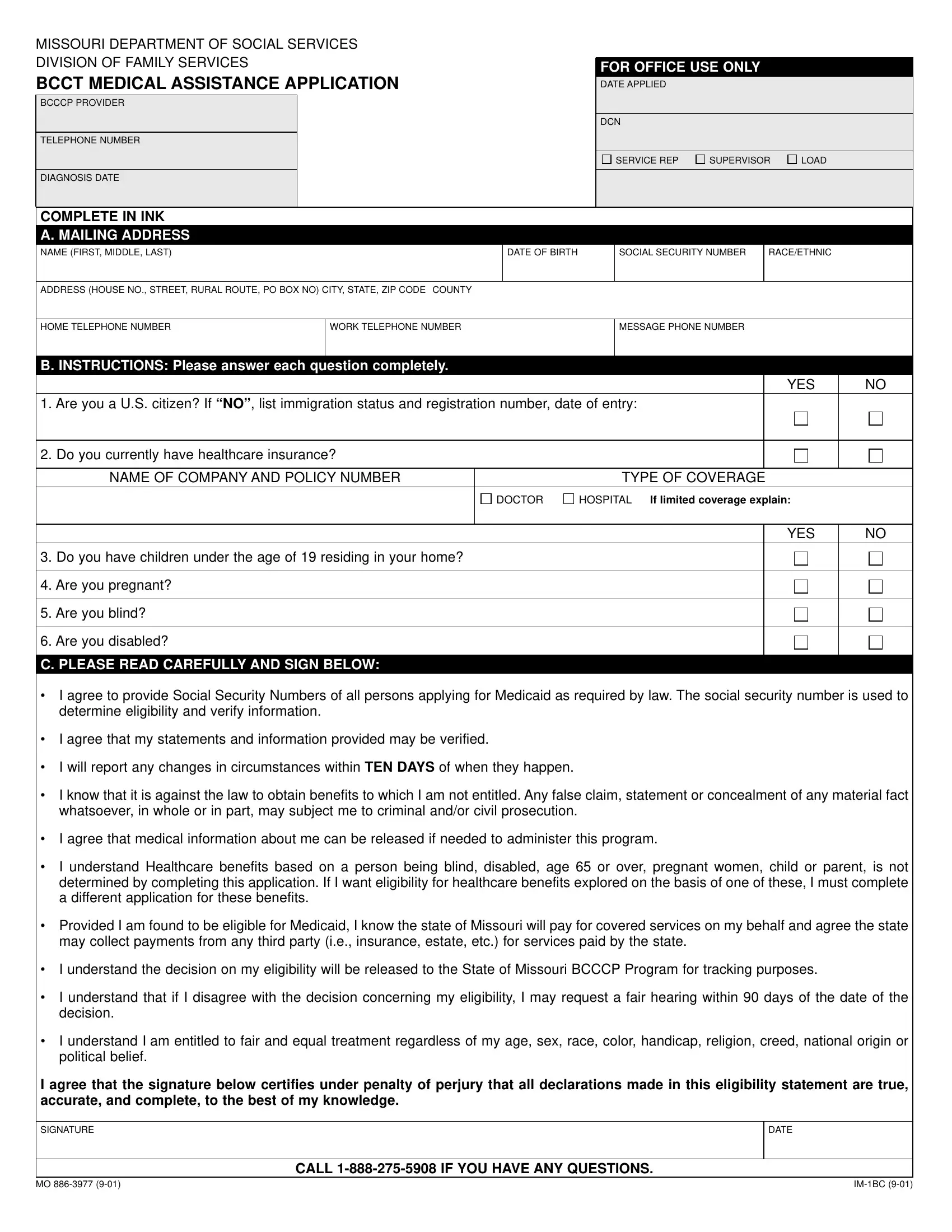
The Mo 886 3977 form, officially known as the Missouri Department of Social Services Division of Family Services BCCT (Breast and Cervical Cancer Treatment) Medical Assistance Application, is a vital document for individuals seeking Medicaid assistance in Missouri, specifically for breast and cervical cancer treatment under the BCCCP (Breast and Cervical Cancer Control Project). This form enables applicants to provide necessary personal information, including their mailing address, date of birth, social security number, and healthcare insurance details. It questions applicants on their citizenship, current healthcare coverage, and whether they have children under 19 residing with them, among other conditions which might affect their eligibility for medical assistance. The form emphasizes the importance of truthfulness and the legal implications of submitting false information. Instructions mandate applicants to report any change in circumstances and agree to the release of medical information for program administration. Importantly, it alerts applicants that eligibility for benefits based on other conditions like disability, age, pregnancy, or parental status requires a different form. The completed application, subject to eligibility determination, acknowledges that the state will recover expenses from any third-party payments. It also reassures applicants of their rights to a fair hearing in case of disagreement with the eligibility decision, emphasizing a commitment to fair and equal treatment irrespective of demographic factors. Contact information for various MC+ Service Centers across Missouri is included, ensuring applicants know where to send their form or seek assistance.
| Question | Answer |
|---|---|
| Form Name | Form Mo 886 3977 |
| Form Length | 2 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 30 sec |
| Other names | im1bc_0901 bcct missouri provider form |
MISSOURI DEPARTMENT OF SOCIAL SERVICES DIVISION OF FAMILY SERVICES
BCCT MEDICAL ASSISTANCE APPLICATION
BCCCP PROVIDER
TELEPHONE NUMBER
DIAGNOSIS DATE
FOR OFFICE USE ONLY
DATE APPLIED
DCN
SERVICE REP |
SUPERVISOR |
LOAD |
COMPLETE IN INK
A. MAILING ADDRESS
NAME (FIRST, MIDDLE, LAST)
DATE OF BIRTH
SOCIAL SECURITY NUMBER
RACE/ETHNIC
ADDRESS (HOUSE NO., STREET, RURAL ROUTE, PO BOX NO) CITY, STATE, ZIP CODE COUNTY
HOME TELEPHONE NUMBER
WORK TELEPHONE NUMBER
MESSAGE PHONE NUMBER
B. INSTRUCTIONS: Please answer each question completely.
|
|
|
YES |
NO |
1. Are you a U.S. citizen? If “NO”, list immigration status and registration number, date of entry: |
|
|
||
|
|
|
|
|
2. Do you currently have healthcare insurance? |
|
|
|
|
|
|
|
|
|
NAME OF COMPANY AND POLICY NUMBER |
|
TYPE OF COVERAGE |
|
|
|
DOCTOR |
HOSPITAL If limited coverage explain: |
|
|
|
|
|
|
|
3.Do you have children under the age of 19 residing in your home?
4.Are you pregnant?
5.Are you blind?
6.Are you disabled?
C. PLEASE READ CAREFULLY AND SIGN BELOW:
YES
NO
•I agree to provide Social Security Numbers of all persons applying for Medicaid as required by law. The social security number is used to determine eligibility and verify information.
•I agree that my statements and information provided may be verified.
•I will report any changes in circumstances within TEN DAYS of when they happen.
•I know that it is against the law to obtain benefits to which I am not entitled. Any false claim, statement or concealment of any material fact whatsoever, in whole or in part, may subject me to criminal and/or civil prosecution.
•I agree that medical information about me can be released if needed to administer this program.
•I understand Healthcare benefits based on a person being blind, disabled, age 65 or over, pregnant women, child or parent, is not determined by completing this application. If I want eligibility for healthcare benefits explored on the basis of one of these, I must complete a different application for these benefits.
•Provided I am found to be eligible for Medicaid, I know the state of Missouri will pay for covered services on my behalf and agree the state may collect payments from any third party (i.e., insurance, estate, etc.) for services paid by the state.
•I understand the decision on my eligibility will be released to the State of Missouri BCCCP Program for tracking purposes.
•I understand that if I disagree with the decision concerning my eligibility, I may request a fair hearing within 90 days of the date of the decision.
•I understand I am entitled to fair and equal treatment regardless of my age, sex, race, color, handicap, religion, creed, national origin or political belief.
I agree that the signature below certifies under penalty of perjury that all declarations made in this eligibility statement are true, accurate, and complete, to the best of my knowledge.
SIGNATURE
DATE
CALL
MO |
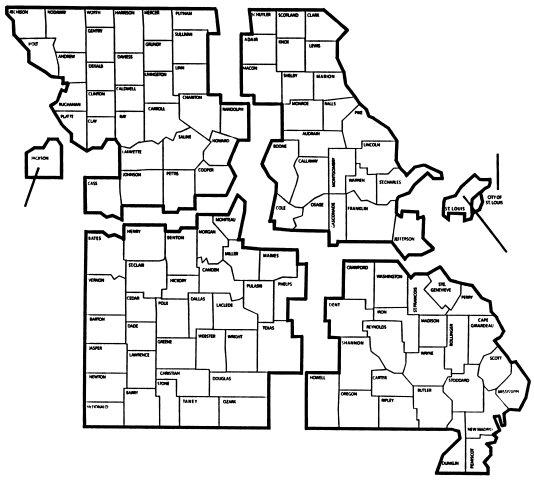
Mail this application to the MC+ Service Center in your Area (see map below).
MC+ Service Center
525 Jules St. #127
St. Joseph, MO 64501
Phone:
Fax:
MC+ Service Center
P.O. Box 318
Troy, MO
Phone:
Fax:
MC+ Service Center
P.O. Box 15188
Kansas City, MO 64106
Phone:
MC+ Service Center
3545 Lindell
St. Louis, MO
Phone:
Fax:
Fax:
MC+ Service Center
9900 Page Avenue
St. Louis, MO 63132
Phone:
Fax:
MC+ Service Center |
MC+ Service Center |
101 Park Central Square |
P.O. Box 578 |
Springfield, MO 65806 |
Cape Girardeau, MO |
Phone: |
Phone: |
Fax: |
Fax: |
MO