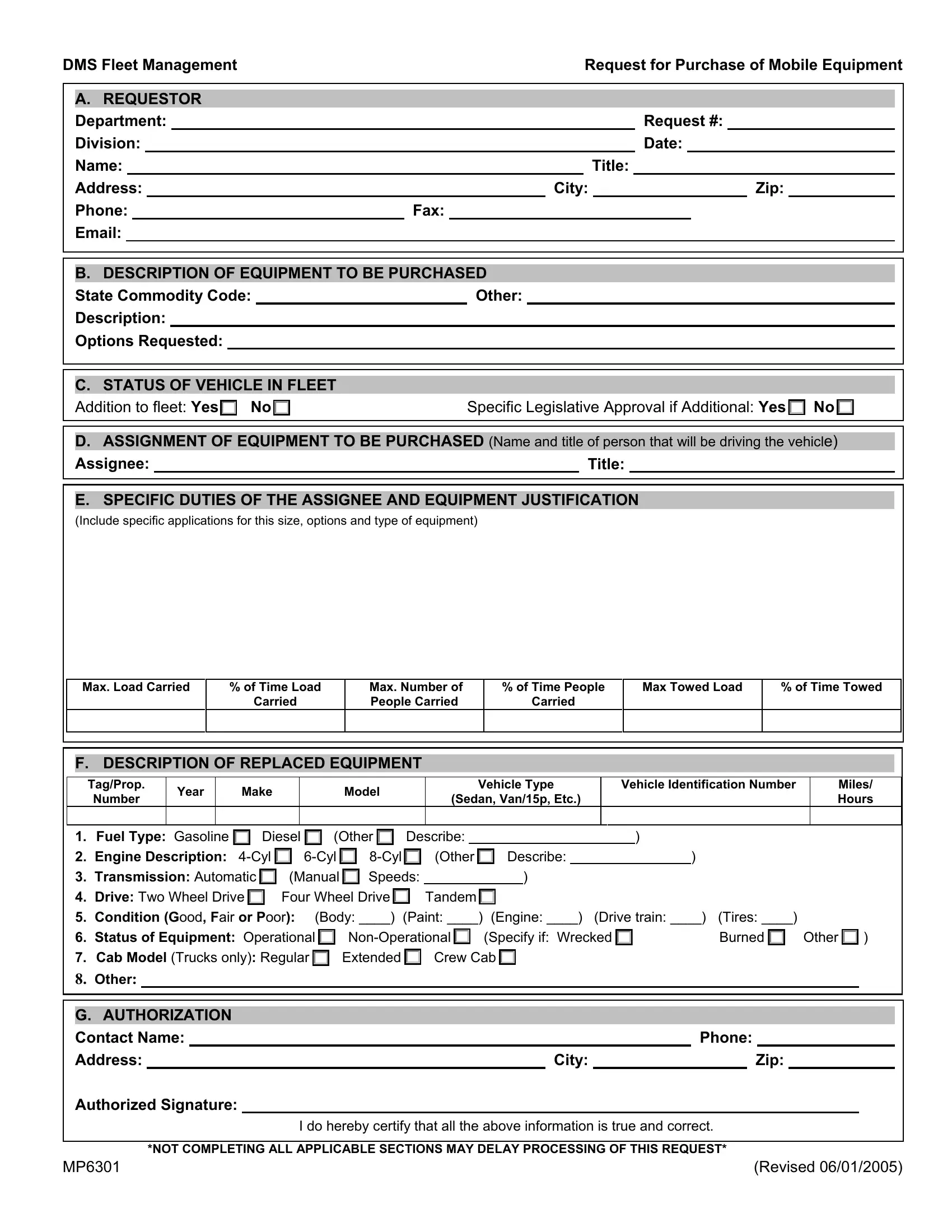
The MP6301 form, known as the DMS Fleet Management Request for Purchase of Mobile Equipment, serves as a critical document within the framework of acquiring vehicles for departmental fleets. This comprehensive form guides the requester through specifying the needs and justification for purchasing new equipment, starting from the fundamental identification of the department, request number, and detailed contact information, to a thorough description of the equipment in question, including state commodity codes, descriptions, and any specific options desired. It further delves into the status of the vehicle within the fleet, distinguishing whether it's an addition or a replacement, and requires legislative approval if it's an additional unit. The assignment section demands identifying who will be using the vehicle, paired with the justification based on specific duties and the equipment’s intended use, offering a granular view on the operational requirements. For replaced equipment, detailed specifications about the previous unit provide a clear comparison to justify the new purchase, touching on everything from fuel type and engine description to the vehicle's overall condition and operational status. The form culminates in an authorization section, necessitating a formal sign-off that all provided information is accurate and complete. Emphasizing the importance of filling out each section meticulously, the MP6301 form underscores the process's integrity for acquiring mobile equipment, ensuring that purchases are justified, well-documented, and aligned with the department's needs.
| Question | Answer |
|---|---|
| Form Name | Form Mp6301 |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | DMS, dms form mp6301, REQUESTOR, 8-Cyl |
DMS Fleet Management |
|
|
|
|
|
|
|
|
|
Request for Purchase of Mobile Equipment |
||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
A. REQUESTOR |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||
|
Department: |
|
|
|
|
|
|
|
|
|
|
|
|
|
Request #: |
|
|
|||||||||||||||
|
Division: |
|
|
|
|
|
|
|
|
|
|
|
|
|
Date: |
|
|
|||||||||||||||
|
Name: |
|
|
|
|
|
|
|
|
|
|
|
Title: |
|
|
|||||||||||||||||
|
Address: |
|
|
|
|
|
|
|
|
|
City: |
|
|
|
|
|
|
Zip: |
|
|
||||||||||||
|
Phone: |
|
|
|
|
|
Fax: |
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||
|
Email: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
B. DESCRIPTION OF EQUIPMENT TO BE PURCHASED |
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||
|
State Commodity Code: |
|
|
Other: |
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||
|
Description: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||
|
Options Requested: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
C. STATUS OF VEHICLE IN FLEET |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||
|
Addition to fleet: Yes |
|
|
No |
X |
|
|
|
Specific Legislative Approval if Additional: Yes |
|
No |
|
|
|||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
D.ASSIGNMENT OF EQUIPMENT TO BE PURCHASED (Name and title of person that will be driving the vehicle)
Assignee:Title:
E. SPECIFIC DUTIES OF THE ASSIGNEE AND EQUIPMENT JUSTIFICATION
(Include specific applications for this size, options and type of equipment)
Max. Load Carried
%of Time Load Carried
Max. Number of People Carried
%of Time People Carried
Max Towed Load
% of Time Towed
F. DESCRIPTION OF REPLACED EQUIPMENT
Tag/Prop.
Number
Year
Make
Model
Vehicle Type
(Sedan, Van/15p, Etc.)
Vehicle Identification Number
Miles/ Hours
1. |
Fuel Type: Gasoline |
|
|
|
Diesel |
|
|
|
|
(Other |
|
|
|
Describe: |
|
|
|
|
|
|
|
|
|
|
) |
|
|
|
|
|
|
|
||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
2. |
Engine Description: |
|
|
|
|
|
|
|
|
|
(Other |
|
|
|
|
|
Describe: |
|
|
) |
|
|
|
|
|
|
||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||
3. |
Transmission: Automatic |
|
|
|
(Manual |
|
|
|
Speeds: |
|
) |
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||
4. |
Drive: Two Wheel Drive |
|
|
|
Four Wheel Drive |
|
|
|
|
Tandem |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||
5. |
Condition (Good, Fair or Poor): |
|
(Body: ____) |
(Paint: ____) |
(Engine: ____) (Drive train: ____) |
(Tires: ____) |
|
|
|
|||||||||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||||
6. |
Status of Equipment: Operational |
|
|
|
|
|
|
|
|
|
|
(Specify if: Wrecked |
|
|
|
|
Burned |
|
|
Other |
|
) |
||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||||||||||
7. |
Cab Model (Trucks only): Regular |
|
|
Extended |
|
|
|
Crew Cab |
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||||||||
8.Other:
G. AUTHORIZATION |
|
|
|
|
|
|
|
|
||
Contact Name: |
|
|
|
|
Phone: |
|
|
|
||
Address: |
|
|
City: |
|
|
Zip: |
|
|||
Authorized Signature: |
|
|
|
|
|
|
|
|
||
|
|
|
I do hereby certify that all the above information is true and correct. |
|
|
|
||||
*NOT COMPLETING ALL APPLICABLE SECTIONS MAY DELAY PROCESSING OF THIS REQUEST*
MP6301 |
(Revised 06/01/2005) |