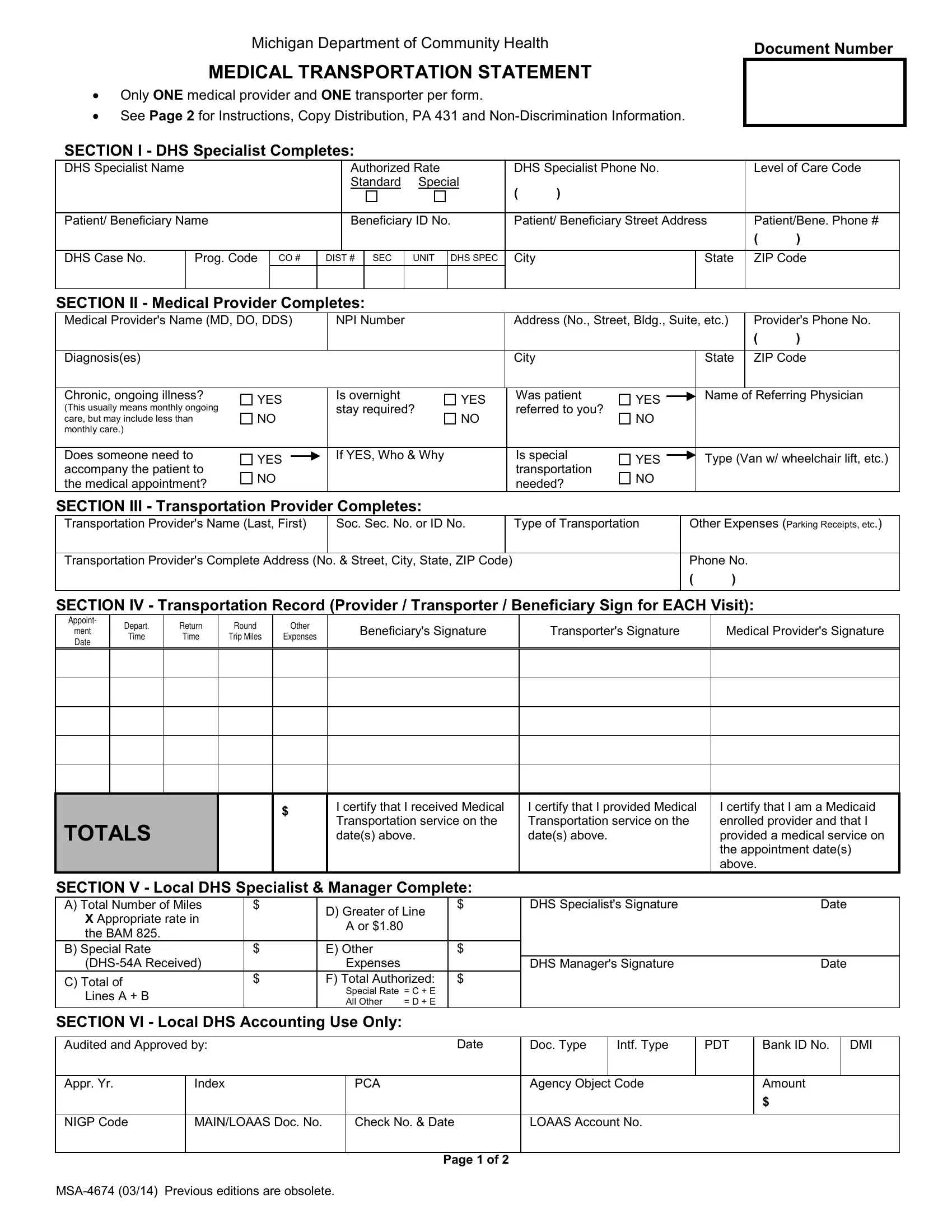
The MSA-4674 form, a crucial document administered by the Michigan Department of Community Health, serves as a standardized method for accounting medical transportation services rendered to beneficiaries, ensuring a seamless process for both medical providers and transporters to claim their services. Tailored specifically to capture instances where only one medical provider and transporter are involved per form, the document demands meticulous completion to facilitate the authorization and payment for medical transportation needs. Given its structured layout, the form aids in streamlining the submission and review of such transportation claims, with distinct sections designated for completion by different stakeholders including DHS Specialists, medical providers, transportation providers, and beneficiaries themselves. The form encompasses details on the service provided - such as diagnosis, type of transportation required, and appointment records - while also outlining instructions for its use, copy distribution, and the critical importance of timely submission within 90 calendar days from the service date. With provisions for documenting each transportation event and a detailed breakdown of incurred costs, the MSA-4674 is instrumental in ensuring accurate reimbursement for transportation services essential for beneficiaries’ medical care, emphasizing the complex interplay between healthcare accessibility and administrative processes.
| Question | Answer |
|---|---|
| Form Name | Form Msa 4674 |
| Form Length | 2 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 30 sec |
| Other names | PCA, DHS, PDT, Intf |
Michigan Department of Community Health |
Document Number |
|
MEDICAL TRANSPORTATION STATEMENT
•Only ONE medical provider and ONE transporter per form.
•See Page 2 for Instructions, Copy Distribution, PA 431 and
SECTION I - DHS Specialist Completes:
DHS Specialist Name |
|
|
|
Authorized Rate |
DHS Specialist Phone No. |
Level of Care Code |
||||||
|
|
|
|
Standard |
Special |
( |
) |
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
||
Patient/ Beneficiary Name |
|
Beneficiary ID No. |
Patient/ Beneficiary Street Address |
Patient/Bene. Phone # |
||||||||
|
|
|
|
|
|
|
|
|
|
|
( |
) |
|
|
|
|
|
|
|
|
|
|
|
|
|
DHS Case No. |
Prog. Code |
CO # |
DIST # |
SEC |
UNIT |
DHS SPEC |
City |
|
State |
ZIP Code |
||
|
|
|
|
|
|
|
|
|
|
|
|
|
SECTION II - Medical Provider Completes:
Medical Provider's Name (MD, DO, DDS) |
NPI Number |
|
|
|
Address (No., Street, Bldg., Suite, etc.) |
|
Provider's Phone No. |
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
( |
) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Diagnosis(es) |
|
|
|
|
|
|
|
City |
|
|
|
|
State |
|
ZIP Code |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
Chronic, ongoing illness? |
|
|
|
Is overnight |
|
|
|
Was patient |
|
|
|
|
Name of Referring Physician |
|||
YES |
YES |
|
YES |
|
|
|||||||||||
(This usually means monthly ongoing |
stay required? |
|
referred to you? |
|
|
|
|
|
|
|||||||
NO |
NO |
|
NO |
|
|
|
|
|
|
|||||||
care, but may include less than |
|
|
|
|
|
|
|
|
|
|||||||
monthly care.) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Does someone need to |
|
|
|
If YES, Who & Why |
|
|
|
Is special |
|
|
|
|
Type (Van w/ wheelchair lift, etc.) |
|||
YES |
|
|
|
YES |
|
|
||||||||||
accompany the patient to |
|
|
|
|
transportation |
|
|
|||||||||
NO |
|
|
|
|
NO |
|
|
|
|
|
|
|||||
the medical appointment? |
|
|
|
|
needed? |
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
SECTION III - Transportation Provider Completes: |
|
|
|
|
|
|
|
|
|
|
|
|
||||
Transportation Provider's Name (Last, First) |
Soc. Sec. No. or ID No. |
|
Type of Transportation |
|
Other Expenses (Parking Receipts, etc.) |
|||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|||||
Transportation Provider's Complete Address (No. & Street, City, State, ZIP Code) |
|
|
|
|
Phone No. |
|
|
|||||||||
|
|
|
|
|
|
|
|
|
|
|
( |
) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
SECTION IV - Transportation Record (Provider / Transporter / Beneficiary Sign for EACH Visit):
Appoint-
ment
Date
Depart.
Time
Return
Time
Round
Trip Miles
Other
Expenses
Beneficiary's Signature
Transporter's Signature
Medical Provider's Signature
TOTALS
$
I certify that I received Medical Transportation service on the date(s) above.
I certify that I provided Medical Transportation service on the date(s) above.
I certify that I am a Medicaid enrolled provider and that I provided a medical service on the appointment date(s) above.
SECTION V - Local DHS Specialist & Manager Complete:
A) Total Number of Miles |
$ |
D) Greater of Line |
$ |
|
X Appropriate rate in |
|
|
||
|
A or $1.80 |
|
|
|
the BAM 825. |
|
|
|
|
|
|
|
|
|
B) Special Rate |
$ |
E) Other |
|
$ |
|
Expenses |
|
|
|
C) Total of |
$ |
F) Total Authorized: |
$ |
|
|
Special Rate |
= C + E |
|
|
Lines A + B |
|
|
||
|
All Other |
= D + E |
|
|
|
|
|
||
DHS Specialist's Signature |
Date |
DHS Manager's Signature |
Date |
SECTION VI - Local DHS Accounting Use Only:
Audited and Approved by: |
|
Date |
Doc. Type |
Intf. Type |
PDT |
Bank ID No. |
DMI |
|
|
|
|
|
|
|
|
|
|
Appr. Yr. |
Index |
PCA |
|
Agency Object Code |
|
Amount |
||
|
|
|
|
|
|
|
$ |
|
|
|
|
|
|
|
|
|
|
NIGP Code |
MAIN/LOAAS Doc. No. |
Check No. & Date |
|
LOAAS Account No. |
|
|
|
|
|
|
|
|
|
|
|
|
|
Page 1 of 2

Instructions for
(Medical Transportation Statement)
GENERAL INSTRUCTIONS:
•Use one form per month for each medical provider or transporter.
•Use this form for 5 or less trips made in a calendar month.
•This form must be returned to the local Michigan Department of Human Services local office within 90 calendar days from the date of service to authorize payment for medical transportation.
COMPLETION INSTRUCTIONS:
SECTION I:
•The DHS Specialist completes this section.
SECTION II:
•The medical provider completes this section. (Only one medical provider per form.)
•Diagnosis is not required if a
SECTION III:
•The transportation provider completes this section.
•Use only ONE transporter per form.
•Leave this section BLANK if the beneficiary drives themselves OR if the beneficiary wishes to receive the transportation payment directly.
SECTION IV - Transportation Record:
Transporter:
•Enter the following for each appointment/visit: date, departure time, return time, number of miles traveled (round trip) and the attendant fee if medically authorized.
•Sign EACH appointment line. This verifies that transportation services were provided on that date.
•If SECTION III was completed, then only that transporter may sign in this section.
Medical Provider (or their staff):
•Confirm the date(s) of appointment(s) and sign your name to verify that the medical visit did occur.
Patient/Beneficiary:
•Sign each appointment line even if you transported yourself. This is also used to verify that each medical appointment was kept and that transportation services were provided.
SECTION V:
•The DHS Specialist calculates the transportation payment and signs their name and dates.
•The DHS Manager reviews the entire form and signs their name approving the payment.
•The local office must then approve the
SECTION VI:
•The local DHS Accounting Unit completes this section.
COPY DISTRIBUTION:
Original:
Copy 1: Copy 2:
•Mail or give this copy to the Beneficiary for completion by the Beneficiary, medical provider and the transporter.
•Return to DHS Specialist for completion. Forward to the local DHS Accounting Unit for payment processing.
•Local DHS Case File copy
•Give this copy to the Beneficiary and/or Transporter.
AUTHORITY: Title XIX of the Social Security Act COMPLETION: Is Voluntary but required if payment from
applicable programs is sought.
The Department of Community Health is an equal opportunity employer, services and programs provider.
Page 2 of 2