MV-145(3-15)
www.dmv.state.pa.us
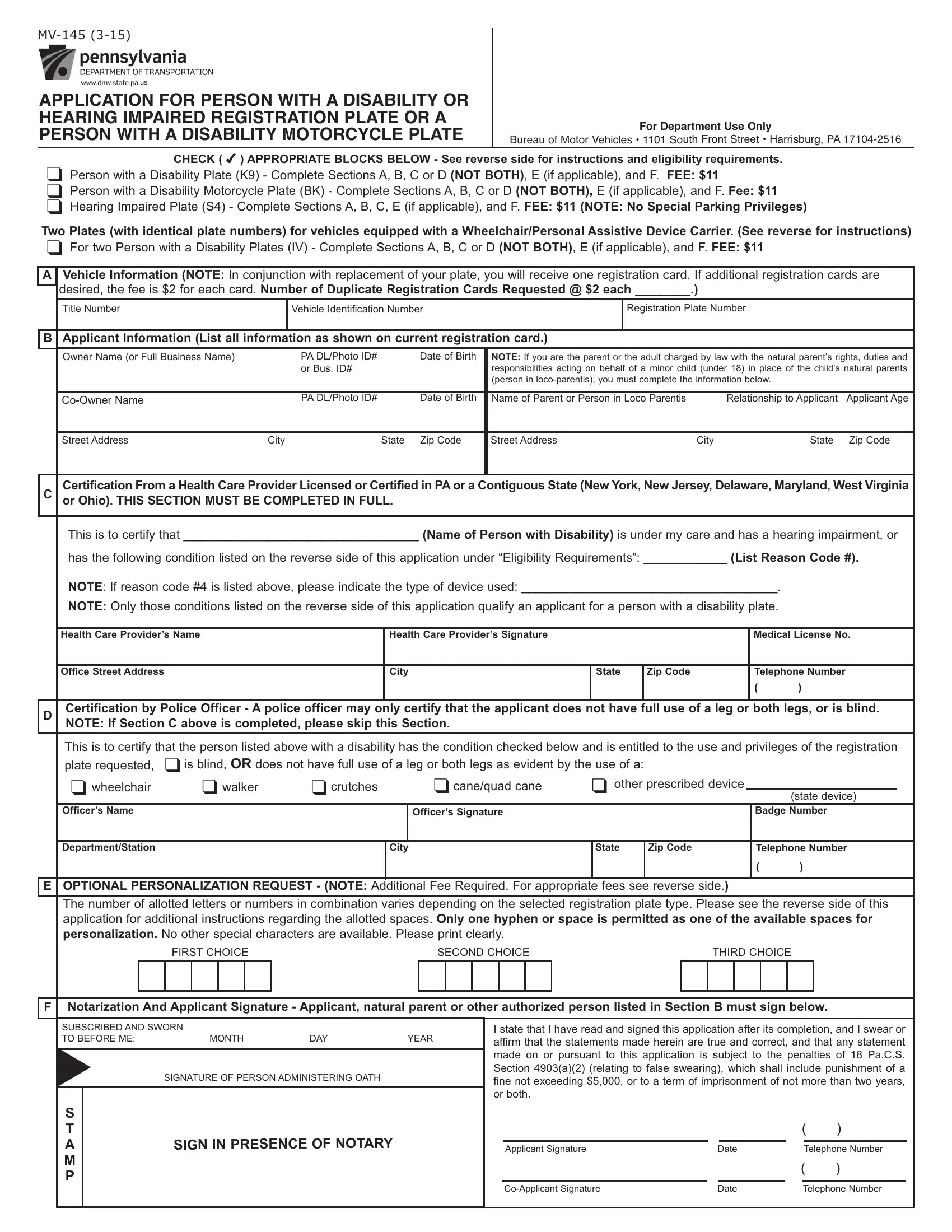
APPLICATION FOR PERSON WITHADISABILITY OR HEARING IMPAIRED REGISTRATION PLATE ORA PERSON WITHADISABILITY MOTORCYCLE PLATE
For Department Use Only Bureau of Motor Vehicles • 1101 South Front Street • Harrisburg, PA 17104-2516
CHECK ( 4) APPROPRIATE BLOCKS BELOW - See reverse side for instructions and eligibility requirements.
qPerson with a Disability Plate (K9) - Complete Sections A, B, C or D (NOT BOTH), E (if applicable), and F. FEE: $11
qPerson with a Disability Motorcycle Plate (BK) - Complete Sections A, B, C or D (NOT BOTH), E (if applicable), and F. Fee: $11
qHearing Impaired Plate (S4) - Complete Sections A, B, C, E (if applicable), and F. FEE: $11(NOTE: No Special Parking Privileges)
Two Plates (with identical plate numbers) for vehicles equipped with a Wheelchair/Personal Assistive Device Carrier. (See reverse for instructions)
qFor two Person with a Disability Plates (IV) - Complete Sections A, B, C or D (NOT BOTH), E (if applicable), and F. FEE: $11
AVehicle Information (NOTE: In conjunction with replacement of your plate, you will receive one registration card. If additional registration cards are desired, the fee is $2 for each card. Number of Duplicate Registration Cards Requested @ $2 each ________.)
Title Number |
Vehicle Identification Number |
Registration Plate Number |
|
|
|
B ApplicantInformation (List all information as shown on current registration card.) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Owner Name (or Full Business Name) |
PA DL/Photo ID# |
|
|
Date of Birth |
NOTE: If you are the parent or the adult charged by law with the natural parent’s rights, duties and |
|
|
|
or Bus. ID# |
|
|
|
responsibilities acting on behalf of a minor child (under 18) in place of the child’s natural parents |
|
|
|
|
|
|
|
(person in loco-parentis), you must complete the information below. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Co-Owner Name |
|
PA DL/Photo ID# |
|
|
Date of Birth |
Name of Parent or Person in Loco Parentis |
Relationship to Applicant |
Applicant Age |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Street Address |
|
City |
State Zip Code |
Street Address |
|
|
City |
State |
Zip Code |
|
|
|
|
|
|
|
|
|
|
C |
CertificationFromaHealthCareProviderLicensedorCertifiedinPAoraContiguousState(NewYork,NewJersey,Delaware,Maryland,WestVirginia |
or Ohio). THIS SECTION MUST BE COMPLETED IN FULL. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
This is to certify that __________________________________ (Name of Person with Disability) is under my care and has a hearing impairment, or |
|
has the following condition listed on the reverse side of this application under “Eligibility Requirements”: ____________ (List Reason Code #). |
|
NOTE: If reason code #4 is listed above, please indicate the type of device used: _____________________________________. |
|
|
|
|
NOTE: Only those conditions listed on the reverse side of this application qualify an applicant for a person with a disability plate. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Health Care Provider’s Name |
|
|
Health Care Provider’s Signature |
|
|
|
|
Medical License No. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Office Street Address |
|
|
|
City |
|
State |
Zip Code |
|
|
Telephone Number |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
( |
) |
|
|
|
|
|
|
|
|
|
|
|
|
D |
Certification by Police Officer - A police officer may only certify that the applicant does not have full use of a leg or both legs, or is blind. |
NOTE: If Section C above is completed, please skip this Section. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
This is to certify that the person listed above with a disability has the condition checked below and is entitled to the use and privileges of the registration |
|
plate requested, |
qis blind, OR does not have full use of a leg or both legs as evident by the use of a: |
|
|
|
|
|
|
|
|
qwheelchair |
qwalker |
qcrutches |
|
|
qcane/quad cane |
q other prescribed device |
|
|
|
|
|
|
|
|
(state device) |
|
Officer’s Name |
|
|
|
|
Officer’s Signature |
|
|
|
|
Badge Number |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Department/Station |
|
|
|
City |
|
State |
Zip Code |
|
|
Telephone Number |
|
|
|
|
|
|
|
|
|
|
|
|
( |
) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
E |
OPTIONAL PERSONALIZATION REQUEST - (NOTE: Additional Fee Required. For appropriate fees see reverse side.) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
The number of allotted letters or numbers in combination varies depending on the selected registration plate type. Please see the reverse side of this application for additional instructions regarding the allotted spaces. Only one hyphen or space is permitted as one of the available spaces for personalization. No other special characters are available. Please print clearly.
|
|
|
FIRST CHOICE |
|
|
|
SECOND CHOICE |
|
|
THIRD CHOICE |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
F |
Notarization And Applicant Signature - Applicant, natural parent or other authorized person listed in Section B must sign below. |
|
|
|
|
|
|
|
|
|
|
SUBSCRIBED AND SWORN |
|
|
|
|
|
|
I state that I have read and signed this application after its completion, and I swear or |
|
TO BEFORE ME: |
|
|
MONTH |
DAY |
YEAR |
|
|
|
affirm that the statements made herein are true and correct, and that any statement |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
t |
|
|
|
|
|
|
|
|
|
|
|
made on or pursuant to this application is subject to the penalties of 18 Pa.C.S. |
|
SIGNATURE OF PERSON ADMINISTERING OATH |
|
|
|
|
|
Section 4903(a)(2) (relating to false swearing), which shall include punishment of a |
|
|
|
|
|
|
fine not exceeding $5,000, or to a term of imprisonment of not more than two years, |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
or both. |
|
|
|
|
|
|
|
SIGN IN PRESENCE OF NOTARY
|
|
|
|
|
|
|
|
|
|
|
( |
) |
|
|
|
|
|
Applicant Signature |
Date |
|
Telephone Number |
|
|
|
|
( |
) |
|
|
|
|
|
|
Co-Applicant Signature |
Date |
|
Telephone Number |
|
Plate Type |
|
Eligibility Requirements |
Qualifying Vehicles |
|
|
Benefits |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
“Reason Codes” |
(1) A passenger vehicle or truck with a |
(1) |
Parking |
permitted |
in |
|
Person with a |
Applicant: |
|
registered gross weight of not more |
spaces designated for disabled |
|
Disability Plate |
(1) |
is blind. |
|
than 14,000 lbs. The vehicle must be |
persons and for 60 minutes in |
|
|
|
|
(2) |
does not have full use of an arm or both arms. |
|
|
used by a person with disability or |
excess of legal parking period |
|
|
(3) |
cannot walk 200 feet without stopping to rest. |
operated exclusively for the use and |
except where local ordinances |
|
|
(4) |
cannotwalkwithouttheuseof,orassistancefrom, |
benefit of the person with a disability. |
or police |
regulations |
provide |
|
|
|
a brace, cane, crutch, another person, prosthetic |
NOTE: Organizations that operate a |
for |
the |
accommodation |
of |
|
|
|
device, wheelchair or other assistive device. |
passenger vehicle to transport persons |
heavy traffic |
during |
morning, |
|
|
(5) |
is restricted by lung disease to such an extent |
with disabilities must supply PennDOT |
afternoon or evening hours. |
|
|
|
|
that the person’s forced (respiratory) expiratory |
with the following: |
(2) Upon request of a person |
|
|
|
volume for one second, when measured by |
a) A notarized statement of how |
with |
disability, |
local authorities |
|
|
|
spirometry, is less than one liter or the arterial |
the vehicle will be used and the |
may erect on the highway as |
|
|
|
oxygen tension is less than 60 MM/HG on room |
type of services that will be |
close as possible to the person’s |
|
|
|
air at rest. |
provided. |
residence |
a sign(s) indicating |
|
|
(6) |
uses portable oxygen. |
that the place is reserved for the |
|
|
b) The weekly or monthly number |
|
|
(7) |
has a cardiac condition to the extent that the |
personwithdisability,thatnoone |
|
|
of hours that the services are |
else |
may |
park there |
unless |
a |
|
|
|
person’s functional limitations are classified in |
|
|
|
provided. |
person with disability |
plate |
or |
|
|
|
severity as Class III or Class IV according to the |
|
|
|
NOTE: The vehicle(s) must be titled in |
placardisdisplayedandthatany |
|
|
|
standards set by the American Heart |
|
|
|
the name of the organization. |
unauthorized |
person |
parking |
|
|
|
Association. |
|
|
|
|
there will be subject to a fine. |
|
|
|
(8) |
is severely limited in his or her ability to walk due |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
to an arthritic, neurological or orthopedic condition. |
|
|
|
|
|
|
|
|
|
(9) |
is a person in loco parentis of a person specified |
|
|
|
|
|
|
|
|
|
|
in paragraph (1), (2), (3), (4), (5), (6), (7) or (8) |
|
|
|
|
|
|
|
|
|
|
above. |
|
|
|
|
|
|
|
|
Definition of Person in Loco Parentis - ANY ADULT charged by law with the natural parent’s rights, duties and responsibilities acting on behalf of a |
|
|
|
|
minor child (under 18) in place of the child’s natural parents. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Hearing Inpaired |
Any person with a hearing impairment verified by |
No restrictions. |
No special benefits. |
|
|
|
Plate |
a licensed health care provider. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Person with a Disability |
Same disabilities as listed for Person with a |
Motorcycle Only. |
Same as above for Person |
|
|
Motorcycle Plate |
Disability Plate. |
|
with a Disability Plate. |
|
|
|
|
|
|
|
|
|
|
|
|
|
•A Health Care Provider is defined as a physician, chiropractor, podiatrist, physician’s assistant or a certified registered nurse practitioner. A Health Care Provider may only certify disabilities within their scope of practice.
•This application may only be used by a vehicle owner or co-owner that qualifies for the type of plate indicated on the front of this application unless the vehicle owner is a person in loco parentis of a qualified person. NOTE: Individuals should list their PA Driver’s License (PA DL) or Photo ID# in the space provided. Businesses should list their Business ID# (Bus. ID) where indicated (i.e. E.I.N.).
•Only one plate issued per qualified person for one vehicle.
•Should you desire to renew your registration in conjunction with this application, you must complete Form MV-140, "Request for Registration," or your registration renewal application and return it with this application along with your annual registration fee and the $11 replacement registration plate fee (if applicable).
•Two registration plates (with identical plate numbers) may be issued for vehicles equipped with a wheelchair/personal assistive device carrier on the rear of the vehicle. One registration plate must be affixed to the rear of the vehicle and one registration plate must be affixed to the rear of the carrier attached to the vehicle for which the plates are issued.
•Send completed application to: Bureau of Motor Vehicles, 1101 S. Front Street, Harrisburg, PA 17104-2516.
IF PERSONALIZING YOUR REGISTRATION PLATE
•Personalized registration plates may contain:
-Person with a Disability registration plates - up to FIVE letters or numbers in combination. An additional $50 fee is required. NOTE: Pre-printed, stacked letter configurations will appear on your personalized registration plate.
-Person with a Disability Motorcycle registration plates - up to THREE letters or numbers in combination. An additional $50 fee is required. NOTE: Pre-printed, stacked letter configurations will appear on your personalized registration plate.
-Hearing Impaired registration plates - up to FIVE letters or numbers in combination. An additional $100 fee is required. NOTE: Pre-printed, stacked letter configuration will appear on your personalized registration plate.
-For two Person with a Disability wheelchair/personal assistive device carrier registration plates, up to FIVE letters or numbers in combination. An additional $50 fee is required. NOTE: Pre-printed, stacked letter configurations will appear on your personalized registration plate.
•If a hyphen or space is used as part of the registration configuration, it counts as one of the available spaces for personalization. Only one hyphen or space is permitted, but not both. NOTE: No additional special characters are available.
•When requesting a numeric character of zero, please list as "Ø" instead of the alpha character of "O".
•PennDOT reserves the right to limit or reject certain requests.
•The fee to personalize your Person with a Disability registration plates is an additional $50. The fee to personalize your Hearing Impaired registration plate is $100. The registration on your vehicle must be current in order for PennDOT to process your request. The additional fee covers the cost of your personalized registration plate order only and will not renew your vehicle's registration. If your registration has expired or expires in the next three months, please include your completed renewal application, Form MV-105, "Pennsylvania Registration RenewalApplication," or Form MV-140, “Request for Registration,” and a separate check or money order in the amount of your registration renewal fee. Payment is to be made by check or money order payable to the Commonwealth of Pennsylvania. PLEASE DO NOT SEND CASH.
•To check personalized registration plate availability, visit PennDOT’s Driver and Vehicle Services website, www.dmv.state.pa.us, and select the Personalized Registration Plate Availability link from the list of services under the Online Driver and Vehicle Services heading. Personalized registration plates will not be reserved until PennDOT receives payment and a completed application, and approves your requested registration plate configuration [number(s) and/or letter(s)]. Please note that registration plate requests are processed on a first-come, first-served basis. Although a requested registration plate configuration may show as being available on the website, it is possible that a request for the same registration plate configuration may have already been submitted by another customer and may not be available when making application.
•Personalized registration plates will be manufactured on the basis of this application. NO REFUND of the fee will be issued when an applicant cancels a request after the order is placed with the manufacturer.
•Allow eight to 10 weeks for delivery.
Visit us at www.dmv.state.pa.us or call us at:
In state: 1-800-932-4600 u TDD: 1-800-228-0676 u Out-of-State: 1-717-412-5300 u TDD Out-of-State: 1-717-412-5380