
When you desire to fill out Dtermination, there's no need to download and install any kind of applications - just give a try to our online PDF editor. To maintain our tool on the forefront of efficiency, we strive to integrate user-driven capabilities and improvements regularly. We are at all times grateful for any feedback - play a vital role in reshaping PDF editing. With a few simple steps, you'll be able to begin your PDF editing:
Step 1: First, access the pdf editor by clicking the "Get Form Button" above on this webpage.
Step 2: With the help of our online PDF editing tool, it is easy to accomplish more than just fill out blanks. Try all the features and make your documents appear great with customized text added, or fine-tune the file's original content to excellence - all that backed up by the capability to incorporate any type of photos and sign the PDF off.
This form will need specific information to be entered, so you should take whatever time to enter exactly what is required:
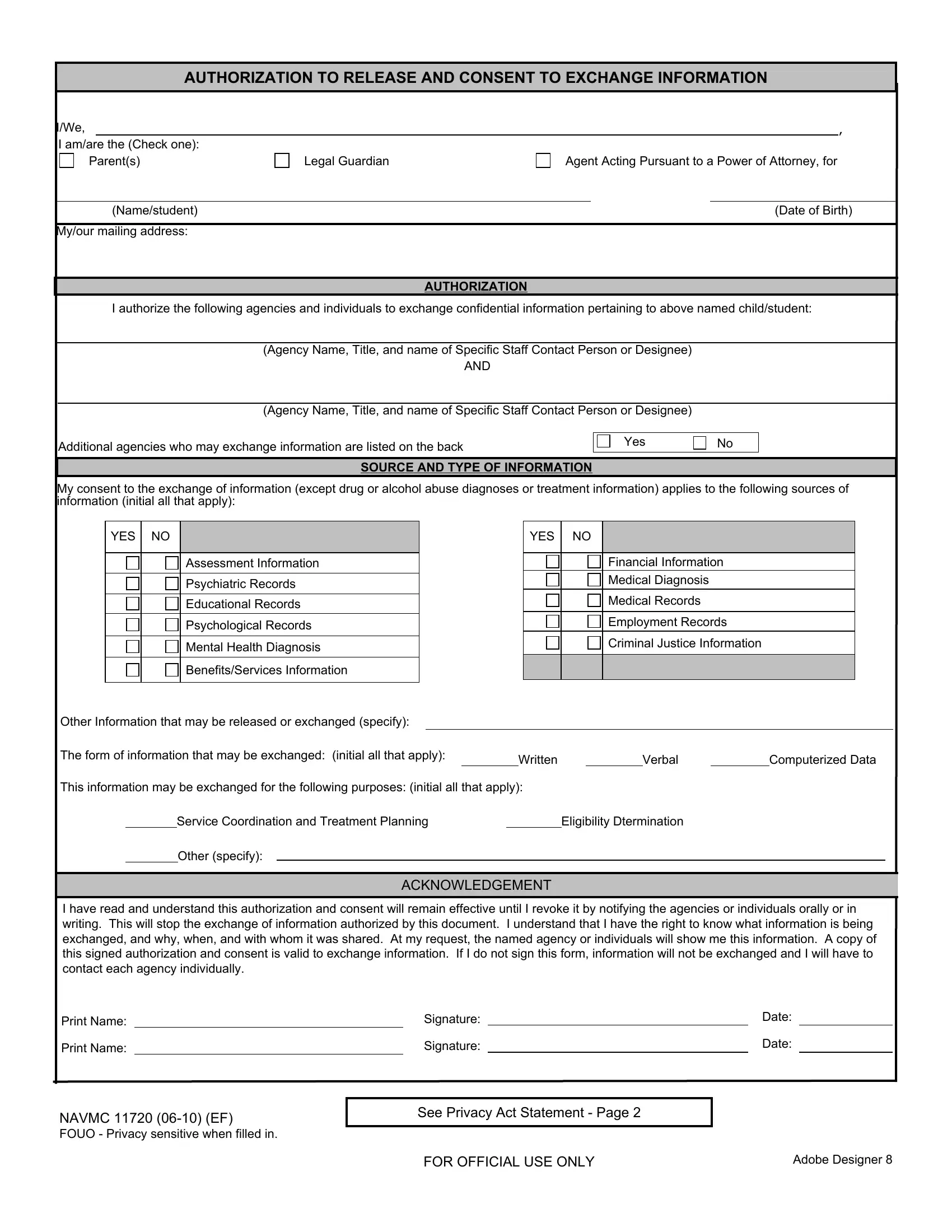
1. Firstly, once filling in the Dtermination, begin with the section with the following fields:
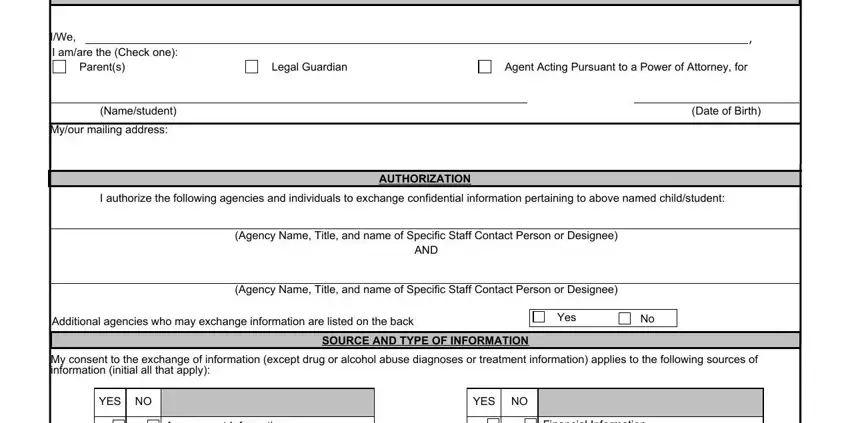
2. Once your current task is complete, take the next step – fill out all of these fields - Assessment Information, Psychiatric Records, Educational Records, Psychological Records, Mental Health Diagnosis, BenefitsServices Information, Financial Information, Medical Diagnosis, Medical Records, Employment Records, Criminal Justice Information, Other Information that may be, The form of information that may, Written, and Verbal with their corresponding information. Make sure to double check that everything has been entered correctly before continuing!
It is easy to make an error while filling in your Employment Records, so be sure you go through it again before you send it in.
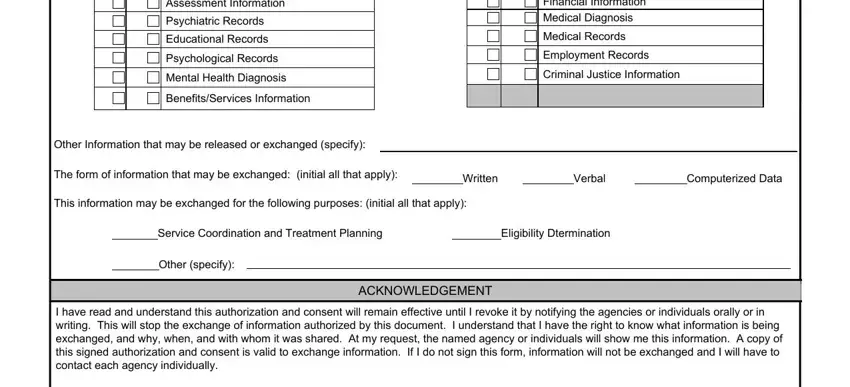
3. The following section is normally quite easy, Print Name, Print Name, Signature, Signature, Date, Date, NAVMC EF FOUO Privacy sensitive, See Privacy Act Statement Page, FOR OFFICIAL USE ONLY, and Adobe Designer - each one of these empty fields is required to be filled out here.
Step 3: Spell-check everything you have typed into the blanks and then click the "Done" button. Right after creating a7-day free trial account with us, you will be able to download Dtermination or send it through email promptly. The form will also be available in your personal account page with your each change. When using FormsPal, you can easily complete forms without needing to be concerned about data incidents or entries getting shared. Our protected software helps to ensure that your private details are maintained safe.