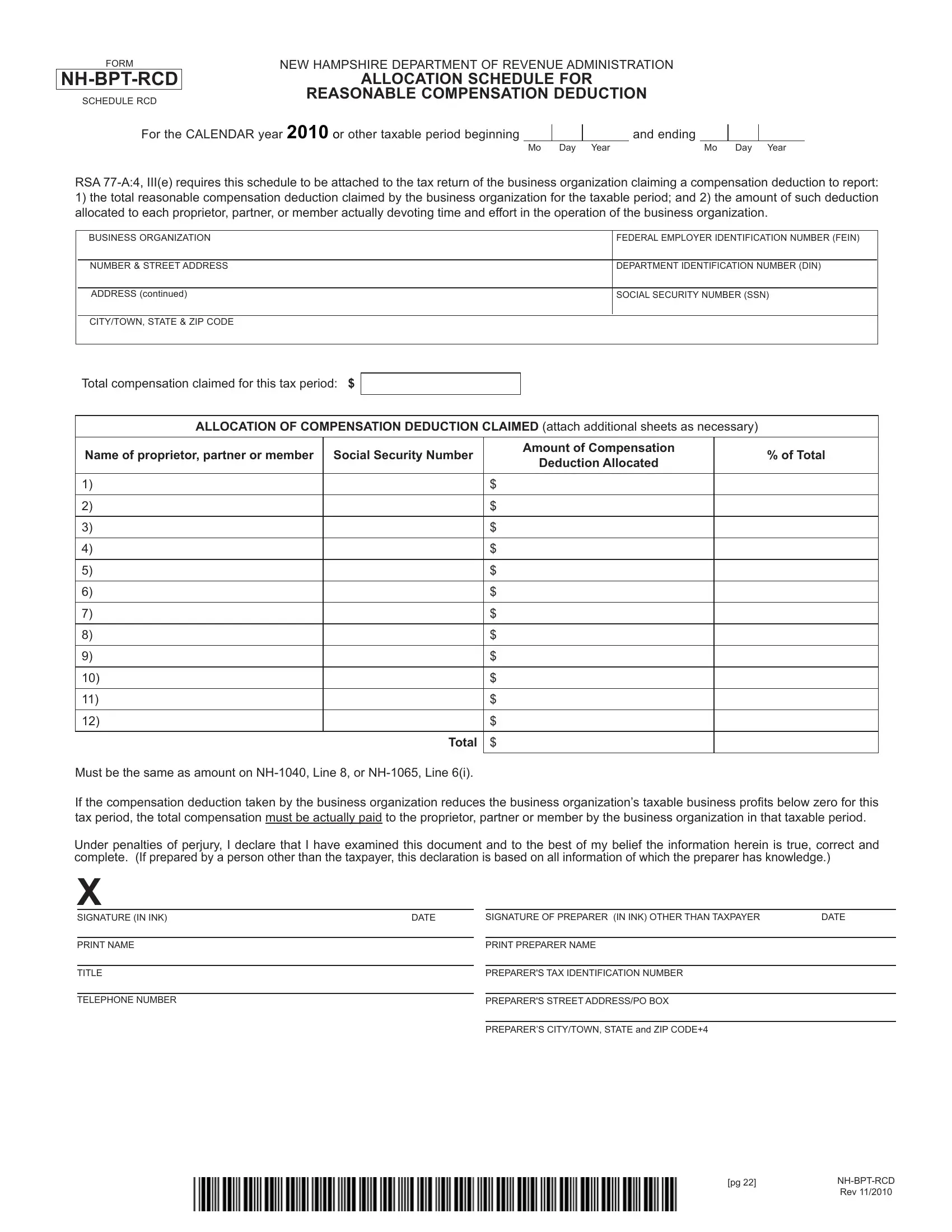
In the intricate landscape of tax deductions, the New Hampshire Department of Revenue Administration offers a specific form that caters to businesses looking to efficiently manage their taxes: the FORM NH-BPT-RCD, Schedule RCD. This particular document plays a crucial role for business organizations during the tax season, especially for the calendar year of 2010 or any other taxable periods specified. Its main purpose is to outline and facilitate the allocation of the reasonable compensation deduction, a tax deduction that is crucial for businesses aiming to accurately report their financial operations. This form demands detailed information about the total compensation deduction claimed, alongside the allocation of this deduction among owners or members actively engaged in the business. It meticulously guides businesses in reporting the distribution of compensation to proprietors, partners, or members, ensuring that the total compensation is not only claimed but also justly allotted based on the individual’s involvement in the business operations. Additionally, this mandate carries the weight of law under RSA 77-A:4, III(e), making it not just a suggestion but a compulsory addition to tax returns for those it concerns. Beyond just a formality, it wraps in layers of legal obligation, accurate financial reporting, and the nuances of tax deductions into a single, vital document for New Hampshire business entities.
| Question | Answer |
|---|---|
| Form Name | Form Nh Bpt Rcd |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | BPT_RCD new hampshire department of revenue bpt return form |
FORM
SCHEDULE RCD
NEW HAMPSHIRE DEPARTMENT OF REVENUE ADMINISTRATION
ALLOCATION SCHEDULE FOR
REASONABLE COMPENSATION DEDUCTION
For the CALENDAR year 2010 or other taxable period beginning
and ending
Mo Day Year |
Mo Day Year |
RSA
1)the total reasonable compensation deduction claimed by the business organization for the taxable period; and 2) the amount of such deduction allocated to each proprietor, partner, or member actually devoting time and effort in the operation of the business organization.
BUSINESS ORGANIZATION
FEDERAL EMPLOYER IDENTIFICATION NUMBER (FEIN)
NUMBER & STREET ADDRESS
DEPARTMENT IDENTIFICATION NUMBER (DIN)
ADDRESS (continued)
SOCIAL SECURITY NUMBER (SSN)
CITY/TOWN, STATE & ZIP CODE
Total compensation claimed for this tax period: $
ALLOCATION OF COMPENSATION DEDUCTION CLAIMED (attach additional sheets as necessary)
Name of proprietor, partner or member |
Social Security Number |
Amount of Compensation |
% of Total |
|
Deduction Allocated |
||||
|
|
|
||
|
|
|
|
|
1) |
|
$ |
|
|
|
|
|
|
|
2) |
|
$ |
|
|
|
|
|
|
|
3) |
|
$ |
|
|
|
|
|
|
|
4) |
|
$ |
|
|
|
|
|
|
|
5) |
|
$ |
|
|
|
|
|
|
|
6) |
|
$ |
|
|
|
|
|
|
|
7) |
|
$ |
|
|
|
|
|
|
|
8) |
|
$ |
|
|
|
|
|
|
|
9) |
|
$ |
|
|
|
|
|
|
|
10) |
|
$ |
|
|
|
|
|
|
|
11) |
|
$ |
|
|
|
|
|
|
|
12) |
|
$ |
|
|
|
|
|
|
|
|
Total |
$ |
|
|
Must be the same as amount on |
|
|
||
|
|
|||
If the compensation deduction taken by the business organization reduces the business organization’s taxable business profits below zero for this tax period, the total compensation must be actually paid to the proprietor, partner or member by the business organization in that taxable period.
Under penalties of perjury, I declare that I have examined this document and to the best of my belief the information herein is true, correct and complete. (If prepared by a person other than the taxpayer, this declaration is based on all information of which the preparer has knowledge.)
X
SIGNATURE (IN INK) |
DATE |
PRINT NAME
TITLE
TELEPHONE NUMBER
SIGNATURE OF PREPARER (IN INK) OTHER THAN TAXPAYER |
DATE |
PRINT PREPARER NAME
PREPARER'S TAX IDENTIFICATION NUMBER
PREPARER'S STREET ADDRESS/PO BOX
PREPARER’S CITY/TOWN, STATE and ZIP CODE+4
[pg 22] |
|
|
Rev 11/2010 |