
You may fill in 122C-3 effectively using our PDFinity® PDF editor. FormsPal professional team is always endeavoring to improve the tool and insure that it is even better for people with its many functions. Take full advantage of present-day innovative opportunities, and discover a trove of unique experiences! With just a couple of easy steps, you can start your PDF journey:
Step 1: Simply click the "Get Form Button" above on this webpage to access our form editing tool. This way, you will find all that is needed to work with your document.
Step 2: Using this advanced PDF tool, you may do more than simply complete blanks. Express yourself and make your forms appear perfect with customized textual content added in, or optimize the file's original input to excellence - all accompanied by the capability to insert your own images and sign it off.
This PDF will need particular information to be filled in, hence you should take some time to fill in what's expected:
1. Start filling out the 122C-3 with a number of necessary blanks. Gather all of the required information and ensure not a single thing forgotten!
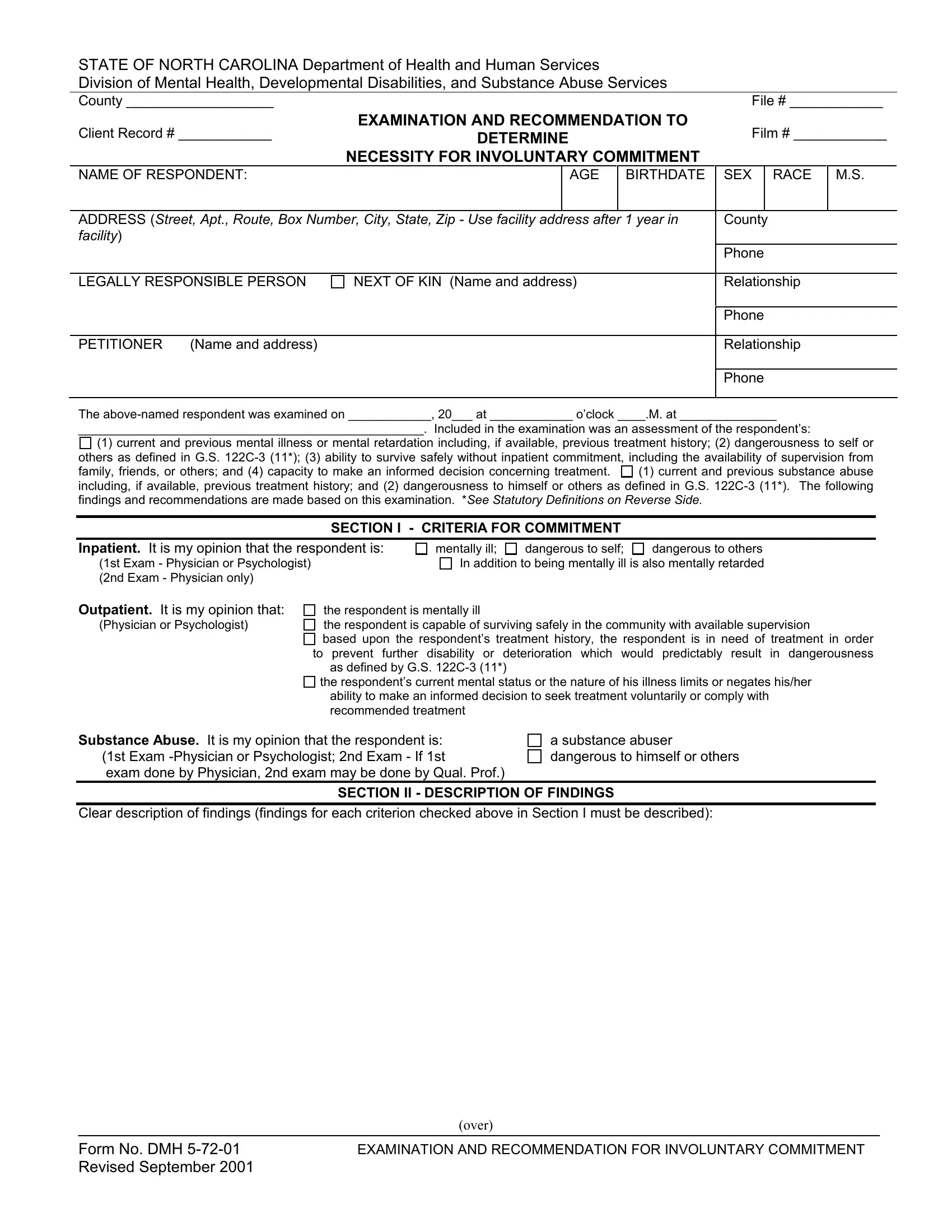
2. Immediately after the last selection of fields is completed, go to type in the applicable information in all these: SECTION I CRITERIA FOR COMMITMENT, Inpatient It is my opinion that, mentally ill, dangerous to others In addition to, dangerous to self, the respondent is mentally ill the, the respondents current mental, ability to make an informed, Substance Abuse It is my opinion, a substance abuser dangerous to, SECTION II DESCRIPTION OF FINDINGS, and Clear description of findings.
Always be very careful while filling in Clear description of findings and mentally ill, because this is the part in which many people make mistakes.
3. This subsequent part should also be quite straightforward, Notable Physical Conditions, ImpressionDiagnosis, Current Medications medical and, SECTION III RECOMMENDATION FOR, Inpatient Commitment for days, Proposed Outpatient Treatment, Substance Abuse Commitment, Release respondent pending hearing, Respondent does not meet the, violent crime including a crime, Respondent or Legally Responsible, Physician Signature, Print Name of Examiner, Original Signature Record, and MD SignatureTitle Eligible - these blanks will have to be filled out here.
4. The fourth part comes with the next few fields to complete: Print Name of Examiner, MD SignatureTitle Eligible, This is to certify that this is a, Address or Facility, City and State, Telephone Number, Address or Facility, Date, Title, STATUTORY DEFINITIONS, and Dangerous to self Within the.
Step 3: Always make sure that your details are right and then simply click "Done" to complete the process. Join FormsPal right now and instantly get 122C-3, available for download. Every edit you make is conveniently kept , which enables you to change the file later when required. Here at FormsPal, we endeavor to be certain that all of your information is kept private.