When individuals in New York State face the challenge of legal blindness, the OCFS-4599 form becomes a pivotal document in their journey towards receiving necessary support and services. Revised in July 2019, this two-page form serves a dual purpose: it is both a report of legal blindness and a request for information from the New York State Commission for the Blind (NYSCB). By meticulously capturing personal information, the condition and cause of blindness, and the patient's vision diagnosis, this form ensures that individuals are accurately registered and receive timely assistance. It not only facilitates the connection between patients and NYSCB for rehabilitation services but also engages healthcare professionals in identifying patients who may benefit from the NYSCB support system. From household task performance to job preparation and retention support, the OCFS-4599 form acts as a bridge to a range of services tailored to meet the unique needs of legally blind individuals in New York State, emphasizing the importance of thorough completion to avoid any delays in the registration process or the receipt of requested information.
| Question | Answer |
|---|---|
| Form Name | Form Ocfs 4599 |
| Form Length | 2 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 30 sec |
| Other names | report for legally blind, report of legal blindness form, legal blindness form 4599, report for legal blindness ny state |
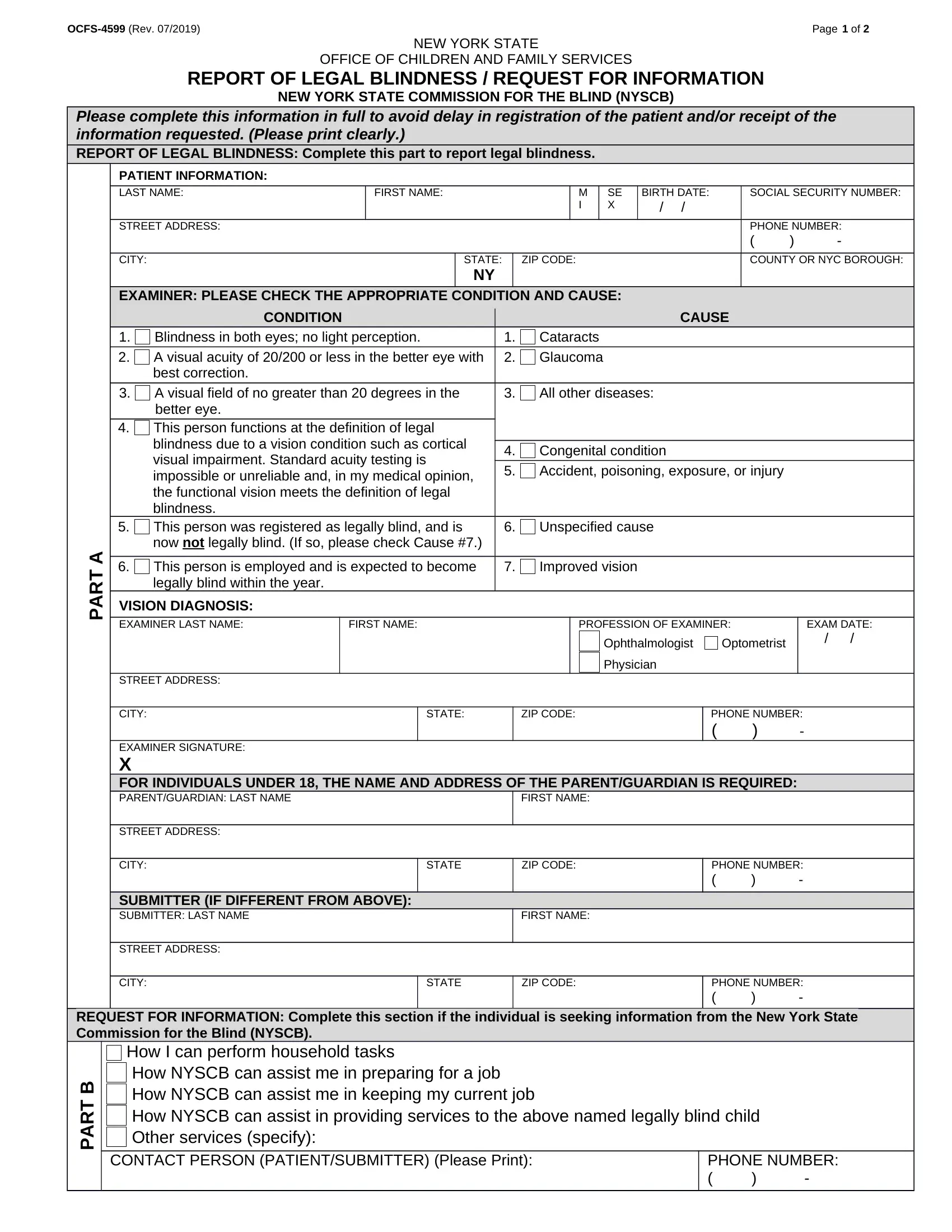
Page 1 of 2 |
NEW YORK STATE
OFFICE OF CHILDREN AND FAMILY SERVICES
REPORT OF LEGAL BLINDNESS / REQUEST FOR INFORMATION
NEW YORK STATE COMMISSION FOR THE BLIND (NYSCB)
Please complete this information in full to avoid delay in registration of the patient and/or receipt of the information requested. (Please print clearly.)
REPORT OF LEGAL BLINDNESS: Complete this part to report legal blindness.
PATIENT INFORMATION:
LAST NAME: |
FIRST NAME: |
M |
SE |
BIRTH DATE: |
SOCIAL SECURITY NUMBER: |
|
|
I |
X |
/ / |
|
STREET ADDRESS: |
|
|
|
|
PHONE NUMBER: |
|
|
|
|
||
|
|
|
|
|
( ) - |
CITY: |
STATE: |
ZIP CODE: |
|
|
COUNTY OR NYC BOROUGH: |
|
NY |
|
|
|
|
EXAMINER: PLEASE CHECK THE APPROPRIATE CONDITION AND CAUSE:
1.
2.
CONDITION |
|
Blindness in both eyes; no light perception. |
1. |
A visual acuity of 20/200 or less in the better eye with |
2. |
best correction. |
|
CAUSE
Cataracts
Glaucoma
3.
4.
5.
A visual field of no greater than 20 degrees in the better eye.
This person functions at the definition of legal blindness due to a vision condition such as cortical visual impairment. Standard acuity testing is impossible or unreliable and, in my medical opinion, the functional vision meets the definition of legal blindness.
This person was registered as legally blind, and is now not legally blind. (If so, please check Cause #7.)
3.
4.
5.
6.
All other diseases:
Congenital condition
Accident, poisoning, exposure, or injury
Unspecified cause
PART A
6. This person is employed and is expected to become |
7. Improved vision |
|
|
|
legally blind within the year. |
|
|
|
|
VISION DIAGNOSIS: |
|
|
|
|
EXAMINER LAST NAME: |
FIRST NAME: |
PROFESSION OF EXAMINER: |
EXAM DATE: |
|
|
|
Ophthalmologist |
Optometrist |
/ / |
|
|
|
||
|
|
Physician |
|
|
STREET ADDRESS: |
|
|
|
|
|
|
|
|
|
CITY: |
STATE: |
ZIP CODE: |
PHONE NUMBER: |
|
|
|
|
( ) - |
|
EXAMINER SIGNATURE: |
|
|
|
|
X |
|
|
|
|
FOR INDIVIDUALS UNDER 18, THE NAME AND ADDRESS OF THE PARENT/GUARDIAN IS REQUIRED: |
|
|||
PARENT/GUARDIAN: LAST NAME |
|
FIRST NAME: |
|
|
|
|
|
|
|
STREET ADDRESS: |
|
|
|
|
|
|
|
|
|
CITY: |
STATE |
ZIP CODE: |
PHONE NUMBER: |
|
|
|
|
( ) - |
|
SUBMITTER (IF DIFFERENT FROM ABOVE): |
|
|
|
|
SUBMITTER: LAST NAME |
|
FIRST NAME: |
|
|
|
|
|
|
|
STREET ADDRESS: |
|
|
|
|
|
|
|
|
|
CITY: |
STATE |
ZIP CODE: |
PHONE NUMBER: |
|
|
|
|
( ) - |
|
REQUEST FOR INFORMATION: Complete this section if the individual is seeking information from the New York State Commission for the Blind (NYSCB).
PART B
How I can perform household tasks
How NYSCB can assist me in preparing for a job How NYSCB can assist me in keeping my current job
How NYSCB can assist in providing services to the above named legally blind child Other services (specify):
CONTACT PERSON (PATIENT/SUBMITTER) (Please Print): |
PHONE NUMBER: |
|
( ) - |

Page 2 of 2 |
REPORT OF LEGAL BLINDNESS (Part A)
(To be completed by ophthalmologist, optometrist or another physician)
This section is to be completed for all persons who meet at least one of the conditions
REQUEST FOR INFORMATION (Part B)
(To be completed by, or for, a legally blind individual)
In addition to completing Part A, please ask your patient if they are experiencing any difficulties performing tasks or activities. If so, please assist or have the patient complete Part B and advise them the form will be forwarded to NYSCB.
Forward the completed form to the NYSCB office listed below that serves the county/borough in which this patient resides. The patient will then be contacted about rehabilitation services.
Counties Served |
Send To: |
Counties Served |
|
|
|
Send To:
Allegany
Cattaraugus
Chautauqua
Erie
Genesee
Livingston
Monroe
Niagara
Ontario
Orleans
Steuben
Wayne
Wyoming
Yates
Albany
Clinton
Columbia
Delaware
Essex
Franklin
Fulton
Greene
Hamilton
Montgomery
Otsego
Rensselaer
Saratoga
Schenectady
Schoharie
St. Lawrence (Adults)
Warren
Washington
NYSCB
Ellicott Square Building
295 Main St.
Suite 545
Buffalo, NY 14203
Phone: (716)
NYSCB
Albany District Office
52 Washington St.
Rensselaer, NY 12144
Phone: (518)
Broome
Cayuga
Chemung
Chenango
Cortland
Herkimer
Jefferson
Lewis
Madison
Oneida
Onondaga
Oswego
Schuyler
Seneca
St Lawrence (Children)
Tioga
Tompkins
Dutchess
Orange
Putnam
Rockland
Sullivan
Ulster
Westchester
Nassau
Suffolk
Queens (Central & Eastern)
Boroughs Served
Brooklyn Manhattan (up to and including 23rd St.)
Staten Island
NYSCB
The Atrium
100 South Salina St.
Suite 105
Syracuse, NY 13202
Phone: (315)
NYSCB
117 East Stevens Ave.
Suite 300
Valhalla, NY 10595
Phone: (914)
NYSCB
711 Stewart Ave.
Suite 210
Garden City, NY 11530
Phone: (516)
NYSCB
80 Maiden Lane
Suite 401
New York, NY 10038
Phone: (212)
Visit our website for additional
information and resources.
visionloss.nv.gov
Bronx
Queens (Western)
Manhattan (North of 23rd
St.)
NYSCB
163 W. 125th St.
Suite 1315
New York, NY 10027
Phone: (212)