
You'll be able to complete Form Ocfs 8018 easily using our PDFinity® online tool. To retain our editor on the cutting edge of convenience, we strive to put into operation user-oriented features and improvements on a regular basis. We're at all times looking for feedback - play a vital role in reshaping PDF editing. In case you are seeking to start, here's what it's going to take:
Step 1: First, access the pdf editor by clicking the "Get Form Button" at the top of this webpage.
Step 2: As you open the file editor, there'll be the document ready to be completed. Aside from filling out different fields, you could also do various other things with the Document, such as adding custom textual content, modifying the initial text, adding images, affixing your signature to the PDF, and much more.
In an effort to complete this form, ensure that you provide the required information in each field:
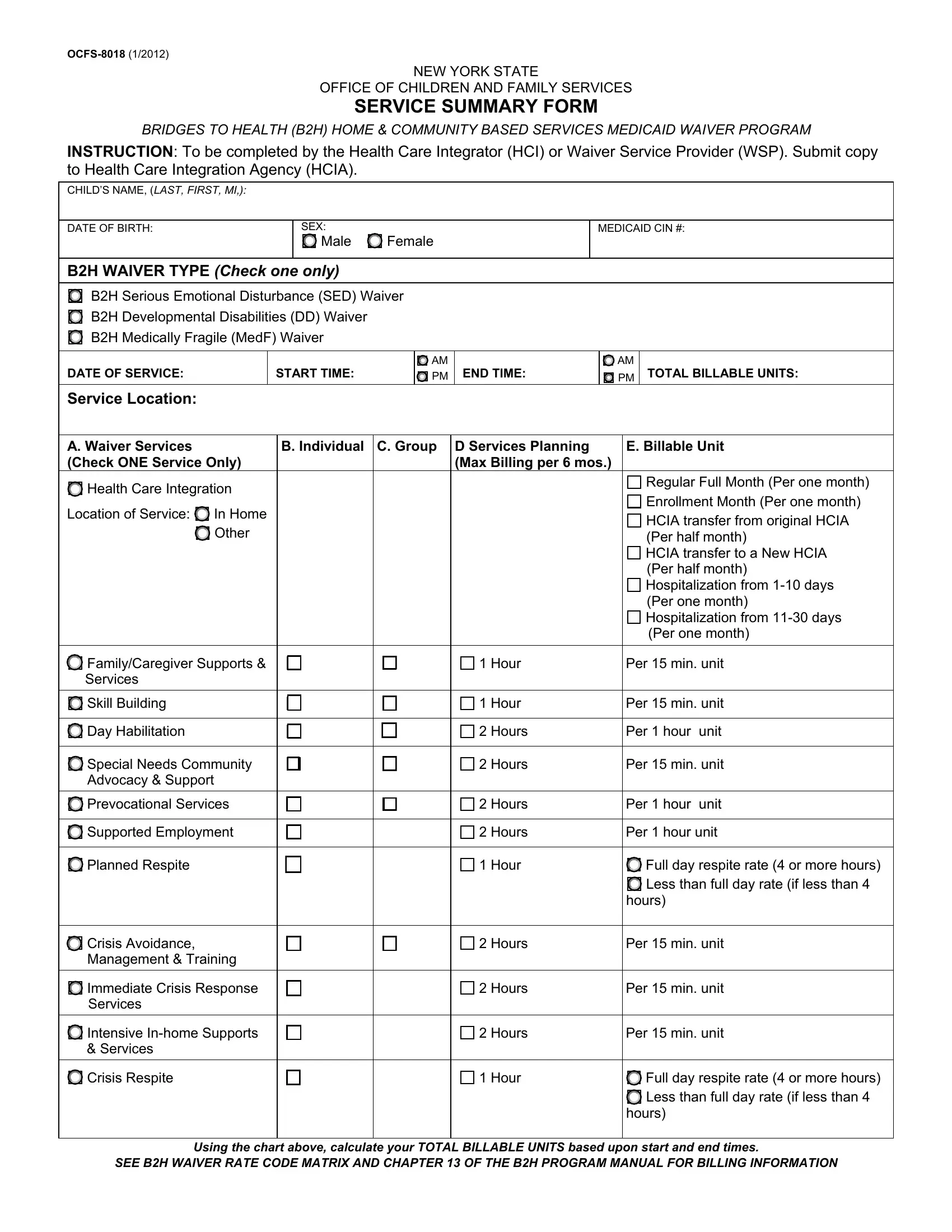
1. Complete the Form Ocfs 8018 with a group of essential blank fields. Note all of the information you need and ensure there's nothing omitted!
2. Once the last array of fields is done, it is time to put in the necessary specifics in FamilyCaregiver Supports Services, Day Habilitation, Special Needs Community Advocacy, Supported Employment, Planned Respite, Crisis Avoidance Management, Immediate Crisis Response Services, Intensive Inhome Supports Services, Hour, Hour, Hours, Hours, Hours, Hours, and Hour so you're able to move on further.
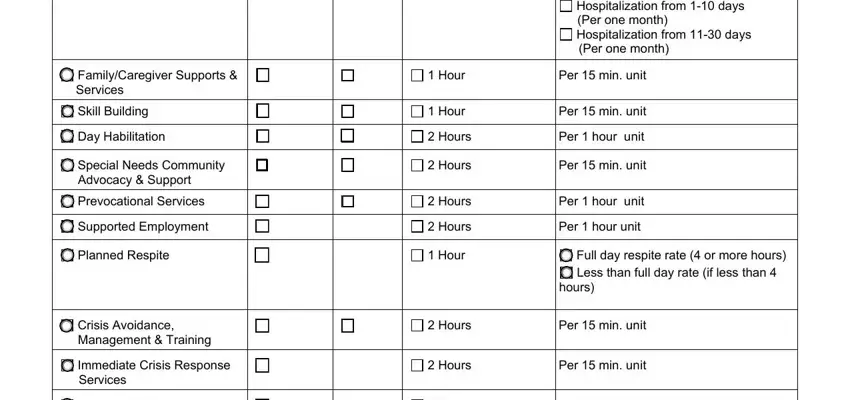
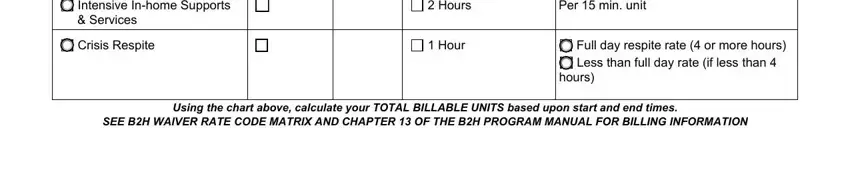
3. Completing Intensive Inhome Supports Services, Crisis Respite, Hours, Hour, Per min unit, Full day respite rate or more, hours, Using the chart above calculate, and SEE BH WAIVER RATE CODE MATRIX AND is essential for the next step, make sure to fill them out in their entirety. Don't miss any details!
4. The following subsection will require your details in the subsequent parts: OCFS Description of service, and Description of childs response to. It is important to provide all of the needed details to go forward.
5. The last section to submit this form is essential. Be sure to fill in the necessary blanks, including My signature verifies that the, CITY, DATE DATE, PHONE STATE, ZIP CODE, NOTE FOR HEALTH CARE INTEGRATION, CONTACT WITH WAIVER SERVICE, Date, CONTACT WITH CASE PLANNERCASE, and Date, before submitting. In any other case, it can result in an incomplete and probably incorrect form!
In terms of ZIP CODE and DATE DATE, make sure you don't make any mistakes in this section. These are certainly the key fields in the document.
Step 3: Before moving on, you should make sure that blank fields were filled in the correct way. The moment you are satisfied with it, click “Done." Grab the Form Ocfs 8018 the instant you register here for a free trial. Quickly gain access to the form from your FormsPal account, along with any modifications and adjustments being all synced! FormsPal offers safe form editing without personal information record-keeping or sharing. Rest assured that your information is in good hands with us!