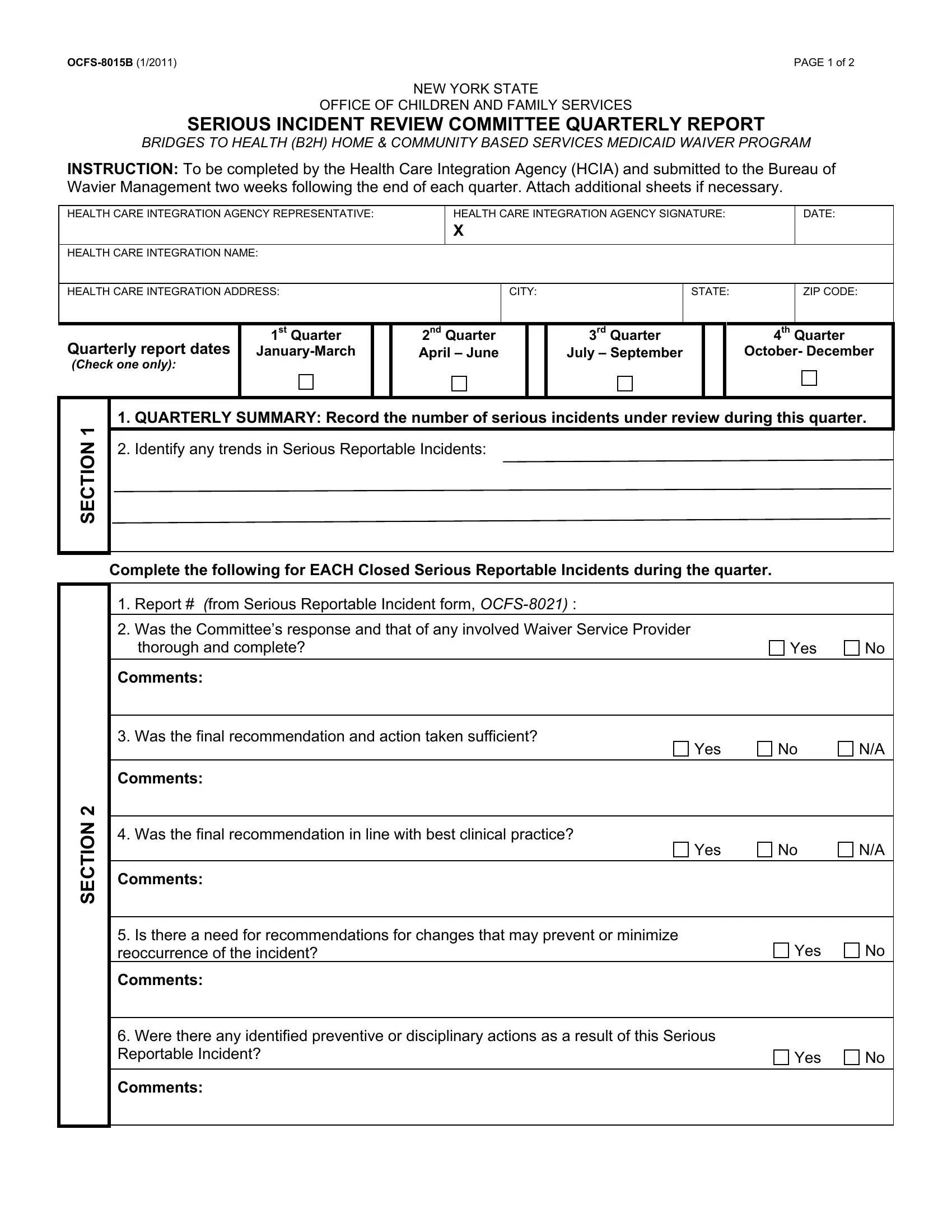
Ensuring the welfare and safety of children within the healthcare system requires diligence and continuous oversight. The OCFS-8015B form serves as a critical tool within this framework, particularly within New York State's Office of Children and Family Services for the Bridges to Health (B2H) Home & Community Based Services Medicaid Waiver Program. This document is designed for completion by Health Care Integration Agencies (HCIA) and must be submitted biannually to the Bureau of Waiver Management. The form is structured to provide a comprehensive overview of serious incidents that have occurred, offering insights into trends of serious reportable incidents, and evaluating the responses and recommendations made by both the review committee and any involved Waiver Service Provider. It seeks detailed assessments regarding whether actions taken were thorough, sufficient, and in alignment with best clinical practices, and importantly, whether there is a need for changes to prevent future occurrences. The form not only facilitates a methodical review of incidents but also encourages accountability and continuous improvement in care standards, making it an indispensable instrument in safeguarding the well-being of children receiving home and community-based services.
| Question | Answer |
|---|---|
| Form Name | Form Ocfs 8015B |
| Form Length | 2 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 30 sec |
| Other names | b2h serious reportable incident form, reoccurrence, OCFS-8021, Wavier |