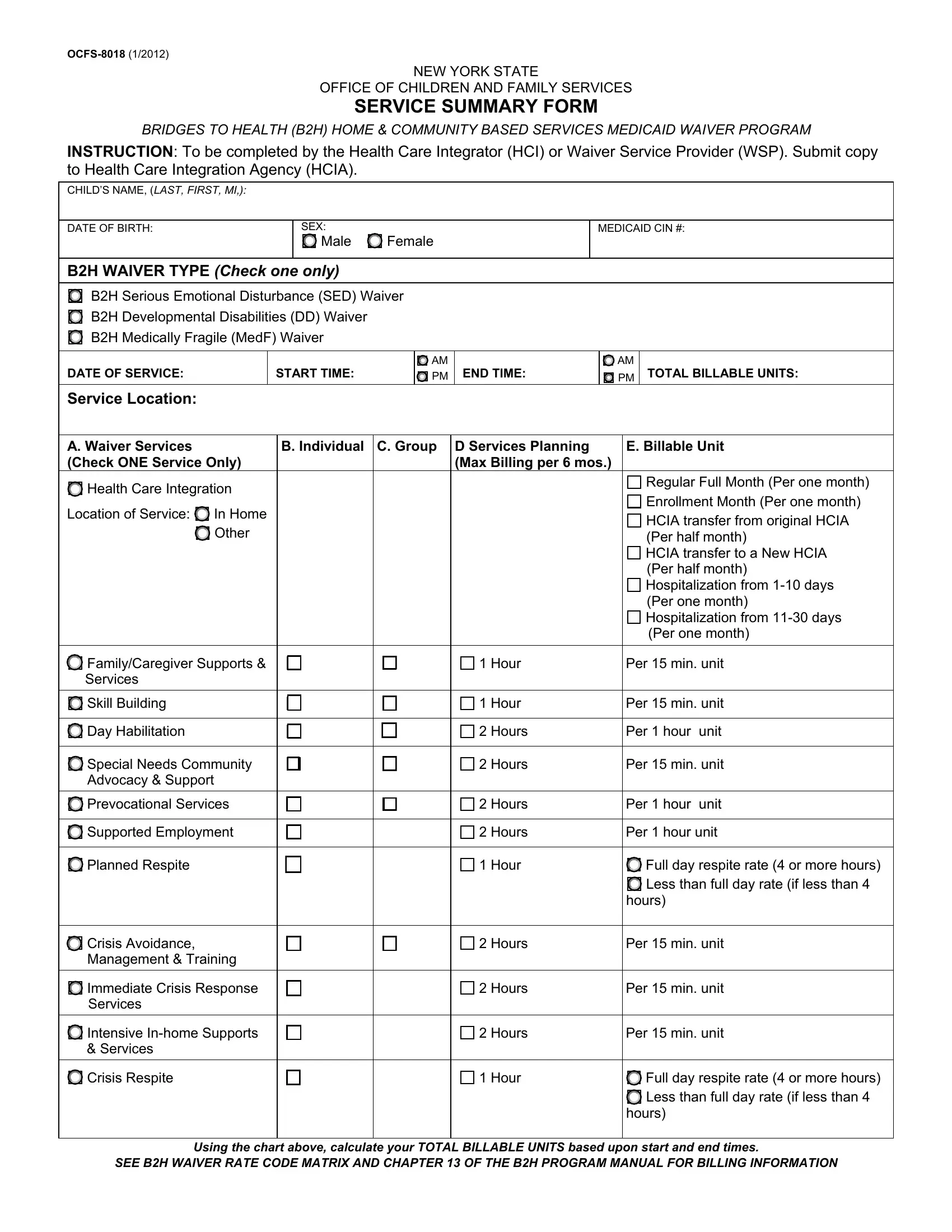
The OCFS-8018 form plays a critical role within New York State's Office of Children and Family Services, specifically within the Bridges to Health (B2H) Home & Community Based Services Medicaid Waiver Program. Designed to be filled out by Health Care Integrators (HCI) or Waiver Service Providers (WSP), this document captures essential information pertaining to the services provided to children under the program. It serves as a comprehensive report, including the child’s name, date of birth, sex, Medicaid CIN #, and the type of B2H Waiver—categorizing the child’s needs as Serious Emotional Disturbance (SED), Developmental Disabilities (DD), or Medically Fragile (MedF). The form further requires documentation of service dates, times, the total billable units, service location, and the specific waiver services provided. Additionally, it compels the service provider to describe the service rendered and the child's response to the intervention, thus tracking progress and ensuring accountability. A notable section requires the signature of both the provider and their supervisor, along with contact information for the Health Care Integration Agency (HCIA), highlighting the collaborative approach in managing the child's healthcare needs. This form is not only an administrative requirement but a critical tool in monitoring the quality and effectiveness of care provided under the B2H program.
| Question | Answer |
|---|---|
| Form Name | Form Ocfs 8018 |
| Form Length | 2 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 30 sec |
| Other names | OCFS 8018 Service Summary Form b2h medicaid payment wsp form |