Ocs Form DD-1 is a document that is used by the United States Office of Personnel Management (OPM) to collect information about an individual's family members. The form is used to determine eligibility for certain benefits, including life insurance and federal employment. The OPM website provides detailed instructions on how to complete the form. It is important to provide accurate and complete information on the form, as it may be used to make decisions about an individual's benefits.
| Question | Answer |
|---|---|
| Form Name | Form Ocs Dd 1 |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | dss tips ocs ofs, louisiana dss, pre, disbursement |
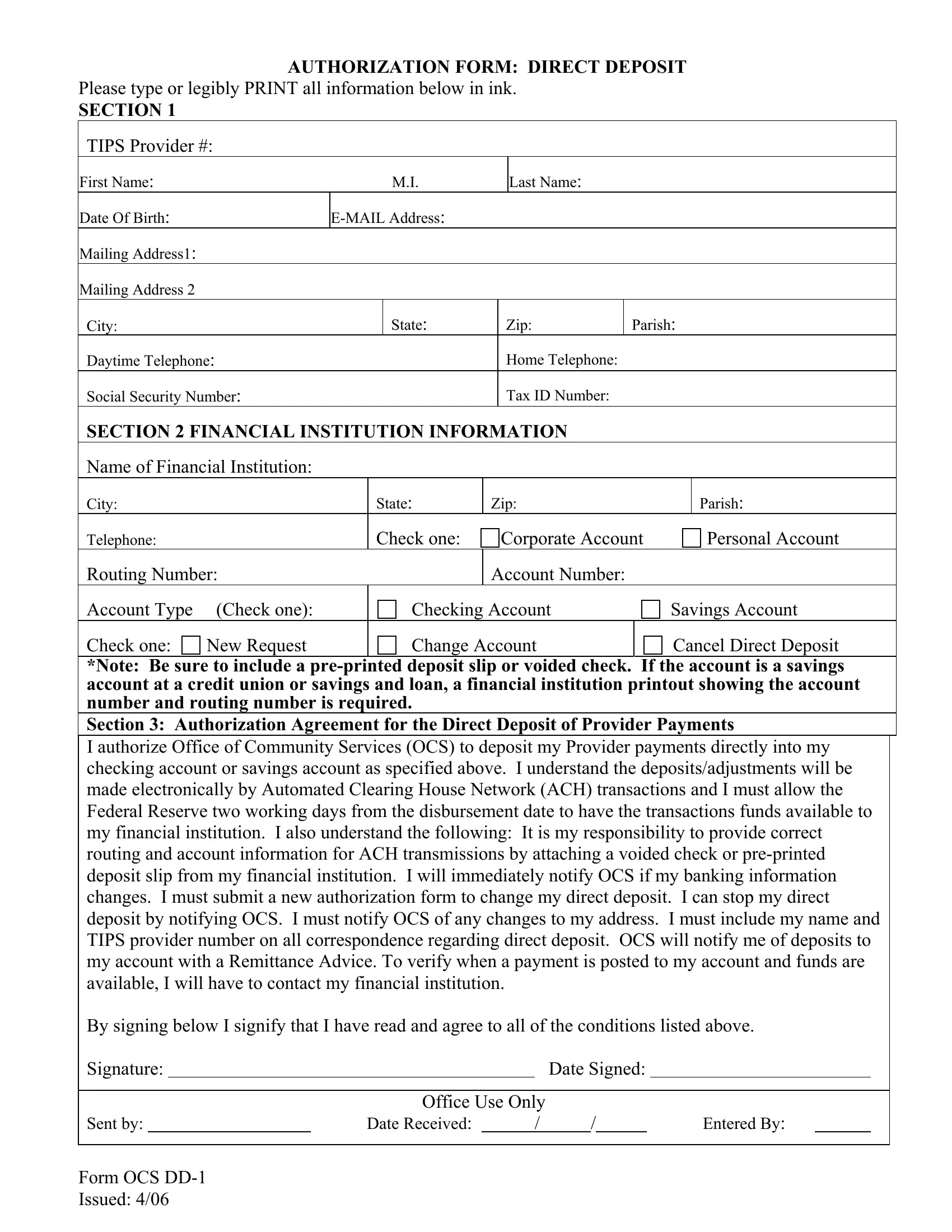
AUTHORIZATION FORM: DIRECT DEPOSIT
Please type or legibly PRINT all information below in ink.
SECTION 1
TIPS Provider #:
First Name: |
|
|
|
M.I. |
|
|
Last Name: |
|
|
|
|
|
Date Of Birth: |
|
|
|
|
|
|
|
|
|
|||
Mailing Address1: |
|
|
|
|
|
|
|
|
|
|
|
|
Mailing Address 2 |
|
|
|
|
|
|
|
|
|
|
|
|
City: |
|
|
|
State: |
|
Zip: |
|
Parish: |
||||
Daytime Telephone: |
|
|
|
|
Home Telephone: |
|
|
|
|
|||
Social Security Number: |
|
|
|
|
Tax ID Number: |
|
|
|
|
|||
SECTION 2 FINANCIAL INSTITUTION INFORMATION |
|
|
|
|
||||||||
Name of Financial Institution: |
|
|
|
|
|
|
|
|
|
|
|
|
City: |
|
|
State: |
Zip: |
|
|
|
Parish: |
||||
Telephone: |
|
|
Check one: |
|
Corporate Account |
|
Personal Account |
|||||
Routing Number: |
|
|
|
Account Number: |
|
|
|
|
||||
Account Type |
(Check one): |
|
|
Checking Account |
|
|
Savings Account |
|||||
Check one: |
New Request |
|
|
Change Account |
|
|
Cancel Direct Deposit |
|||||
*Note: Be sure to include a
Section 3: Authorization Agreement for the Direct Deposit of Provider Payments
I authorize Office of Community Services (OCS) to deposit my Provider payments directly into my checking account or savings account as specified above. I understand the deposits/adjustments will be made electronically by Automated Clearing House Network (ACH) transactions and I must allow the Federal Reserve two working days from the disbursement date to have the transactions funds available to my financial institution. I also understand the following: It is my responsibility to provide correct routing and account information for ACH transmissions by attaching a voided check or
By signing below I signify that I have read and agree to all of the conditions listed above.
Signature: |
|
|
|
|
Date Signed: |
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
Office Use Only |
|
|
|
|
|
|
|
||
Sent by: |
|
|
Date Received: |
|
/ |
/ |
|
|
Entered By: |
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
Form OCS
Issued: 4/06