


west virginia workers compensation disease can be filled out with ease. Just open FormsPal PDF tool to complete the task quickly. Our team is relentlessly endeavoring to improve the tool and insure that it is even easier for people with its extensive features. Discover an ceaselessly innovative experience today - take a look at and find out new possibilities as you go! It merely requires a few easy steps:
Step 1: Click on the orange "Get Form" button above. It'll open our tool so you can begin filling out your form.
Step 2: As you start the online editor, you will find the document made ready to be filled in. Apart from filling out different blanks, it's also possible to perform some other actions with the Document, particularly writing custom text, changing the initial textual content, inserting images, signing the document, and much more.
With regards to the fields of this precise PDF, here is what you should know:
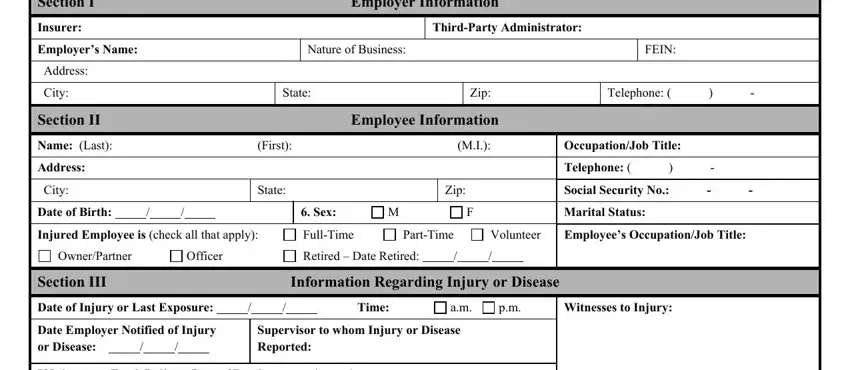
1. Begin completing your west virginia workers compensation disease with a number of essential blank fields. Note all the important information and ensure not a single thing missed!
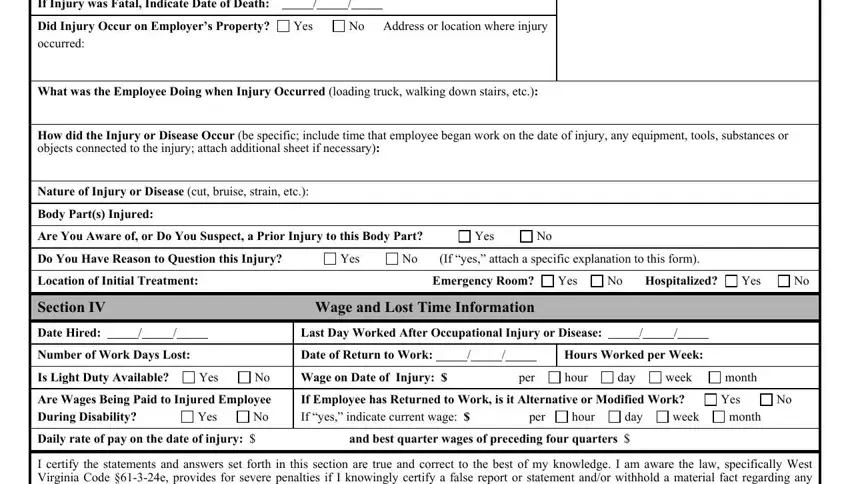
2. Once the previous section is completed, you need to insert the essential details in If Injury was Fatal Indicate Date, Did Injury Occur on Employers, Yes, No Address or location where injury, What was the Employee Doing when, How did the Injury or Disease, Nature of Injury or Disease cut, Body Parts Injured, Are You Aware of or Do You Suspect, Yes, Do You Have Reason to Question, Yes, No If yes attach a specific, Location of Initial Treatment, and Emergency Room allowing you to go to the third step.
3. This part will be hassle-free - fill out every one of the empty fields in I certify the statements and, Print Name, Signature, Title, and Date in order to finish the current step.

It's simple to make a mistake while filling in your Signature, therefore make sure you take another look before you decide to submit it.
Step 3: Before finalizing this file, double-check that all blanks were filled out as intended. Once you determine that it's correct, press “Done." Make a 7-day free trial account at FormsPal and get direct access to west virginia workers compensation disease - download, email, or change from your personal cabinet. FormsPal provides risk-free document editing without personal information recording or sharing. Feel comfortable knowing that your information is in good hands with us!