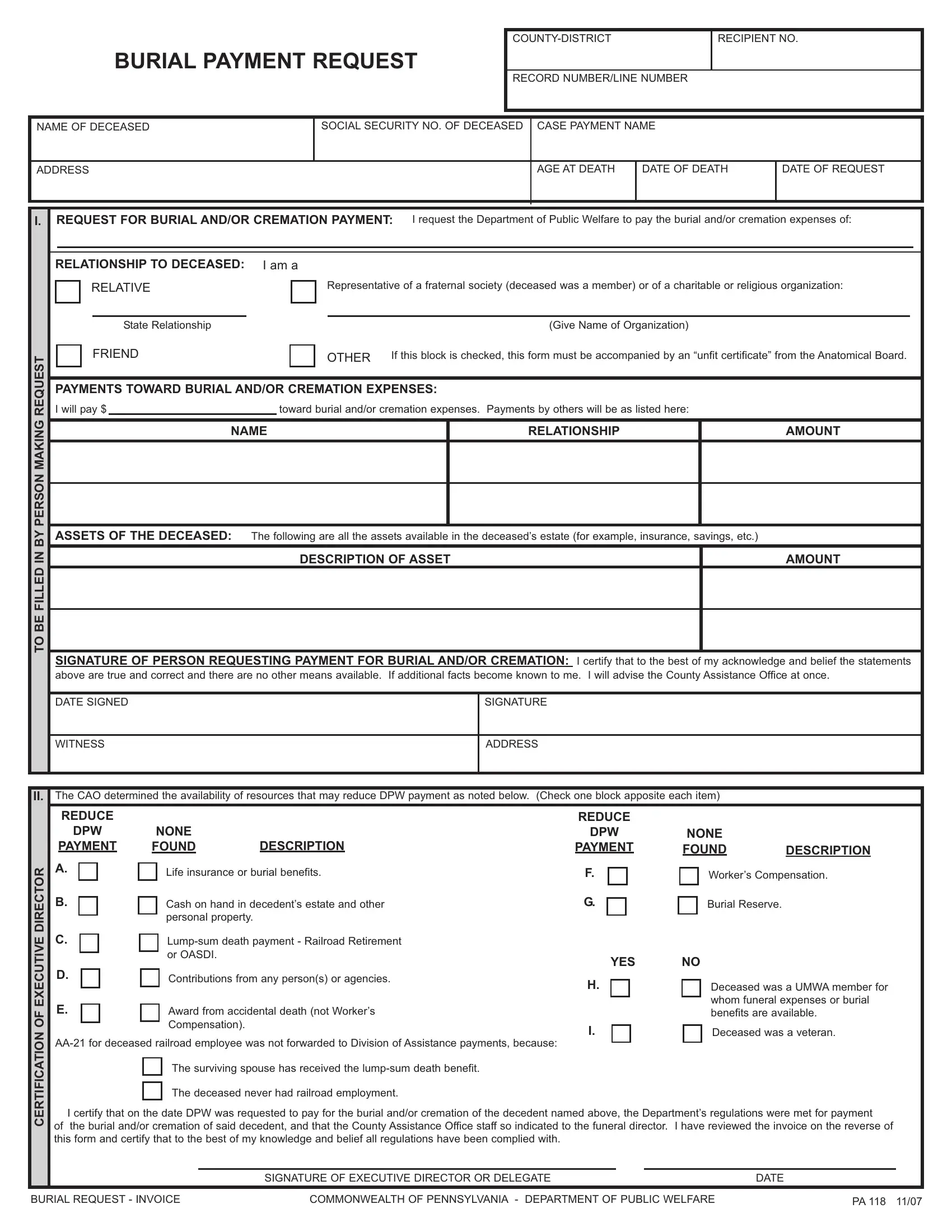
When individuals pass away without the means to pay for their funeral expenses, the Commonwealth of Pennsylvania provides a semblance of dignity in death through the PA 118 form, a Burial Payment Request. This critical document bridges the gap for families and representatives, encompassing a range of applicants - from relatives to fraternal society agents, carrying the heavy burden of arranging a decent farewell for the deceased. It meticulously captures essential details such as the deceased's personal information, the relationship of the requester to the deceased, the financial contribution towards burial or cremation expenses by the requester and others, and lists all accessible assets in the deceased's estate. Additionally, it requires the requestor to attest to the accuracy and completeness of the information provided, with a space for the signature of a witness to these declarations. On the flip side, the form doubles as an invoice for the funeral director to fill out, ensuring that the Pennsylvania Department of Public Welfare (DPW) covers no more than the stipulated amount, less any reductions from available resources or contributions towards the total expense, thereby streamlining the process. This comprehensive approach ensures a clear outline of responsibilities and available support, acknowledging the financial strain funeral costs can impose, while upholding respect for the deceased and their family during a time of loss.
| Question | Answer |
|---|---|
| Form Name | Form Pa 118 |
| Form Length | 2 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 30 sec |
| Other names | pa 118 form burial payment request, DPW, pa118 form social security, form pa 118 |
BURIALPAYMENT REQUEST
|
|
|
|
|
|
|
|
|
RECIPIENTNO. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
RECORD NUMBER/LINE NUMBER
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
NAME OF DECEASED |
|
|
|
|
|
|
|
SOCIALSECURITYNO. OF DECEASED |
|
|
CASE PAYMENTNAME |
|
|
|
|
|
|
||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
ADDRESS |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
AGE ATDEATH |
|
|
DATE OF DEATH |
|
|
|
DATE OF REQUEST |
|
|
|
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||||||||||||
I. |
|
REQUEST FOR BURIALAND/OR CREMATION PAYMENT: I request the Department of Public Welfare to pay the burial and/or cremation expenses of: |
||||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
RELATIONSHIPTO DECEASED: I am a |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||
|
|
|
|
RELATIVE |
|
|
|
|
|
|
|
Representative of a fraternal society (deceased was a member) or of a charitable or religious organization: |
||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
State Relationship |
|
|
|
|
|
|
|
|
|
|
(Give Name of Organization) |
|
|
|
|
|
|||||||||||||
REQUEST |
|
|
|
FRIEND |
|
|
|
|
|
|
|
OTHER If this block is checked, this form must be accompanied by an “unfit certificate” from the Anatomical Board. |
||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||
|
PAYMENTS TOWARD BURIALAND/OR CREMATION EXPENSES: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||
|
I will pay $ |
|
|
|
|
|
toward burial and/or cremation expenses. Payments by others will be as listed here: |
|
|
|
|
|
||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||||
MAKING |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||
|
|
|
|
|
|
|
|
NAME |
|
|
RELATIONSHIP |
|
|
|
|
|
|
|
AMOUNT |
|||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
IN BYPERSON |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||
|
ASSETS OF THE DECEASED: |
The following are all the assets available in the deceased’s estate (for example, insurance, savings, etc.) |
|
|
|
|
|
|||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
DESCRIPTION OF ASSET |
|
|
|
|
|
|
|
|
|
|
|
|
AMOUNT |
||||||||||||
TOBE FILLED |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
SIGNATURE OF PERSON REQUESTING PAYMENT FOR BURIALAND/OR CREMATION: I certify that to the best of my acknowledge and belief the statements |
|||||||||||||||||||||||||||||||||
|
|
|
above are true and correct and there are no other means available. If additional facts become known to me. I will advise the County Assistance Office at once. |
|||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||
|
|
|
DATE SIGNED |
|
|
|
|
|
|
|
|
|
|
SIGNATURE |
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||
|
|
|
WITNESS |
|
|
|
|
|
|
|
|
|
|
ADDRESS |
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||||
II. |
The CAO determined the availability of resources that may reduce DPW payment as noted below. (Check one block apposite each item) |
|
|
|
|
|
||||||||||||||||||||||||||||||
|
|
|
REDUCE |
|
|
|
|
|
|
|
|
|
|
|
|
|
REDUCE |
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
|
|
DPW |
NONE |
|
|
|
|
|
|
|
|
|
|
DPW |
|
|
NONE |
|
|
|
|
|
|||||||||||||
|
|
|
PAYMENT |
FOUND |
DESCRIPTION |
|
|
PAYMENT |
|
|
FOUND |
DESCRIPTION |
||||||||||||||||||||||||
DIRECTOR |
|
A. |
|
Life insurance or burial benefits. |
|
|
F. |
|
|
|
Worker’s Compensation. |
|||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||||
|
B. |
|
Cash on hand in decedent’s estate and other |
|
|
G. |
|
|
|
Burial Reserve. |
|
|
|
|
|
|||||||||||||||||||||
|
|
|
|
|
|
|
personal property. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
EXECUTIVE |
|
C. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||
|
|
|
|
|
|
|
or OASDI. |
|
|
|
|
|
|
|
|
|
|
YES |
|
|
NO |
|
|
|
|
|
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||
|
D. |
|
Contributions from any person(s) or agencies. |
|
|
H. |
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
Deceased was a UMWAmember for |
||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||
|
E. |
|
Award from accidental death (not Worker’s |
|
|
|
|
|
|
|
|
whom funeral expenses or burial |
||||||||||||||||||||||||
OF |
|
|
|
|
|
|
|
|
|
|
benefits are available. |
|||||||||||||||||||||||||
|
|
|
|
|
|
|
Compensation). |
|
|
|
|
|
|
|
|
|
|
I. |
|
|
|
Deceased was a veteran. |
||||||||||||||
CERTIFICATION |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||
|
|
|
|
|
|
|
The surviving spouse has received the |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||
|
|
|
|
|
|
|
The deceased never had railroad employment. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||
|
I certify that on the date DPW was requested to pay for the burial and/or cremation of the decedent named above, the Department’s regulations were met for payment |
|||||||||||||||||||||||||||||||||||
of the burial and/or cremation of said decedent, and that the County Assistance Office staff so indicated to the funeral director. I have reviewed the invoice on the reverse of |
||||||||||||||||||||||||||||||||||||
|
|
|||||||||||||||||||||||||||||||||||
|
|
this form and certify that to the best of my knowledge and belief all regulations have been complied with. |
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
SIGNATURE OF EXECUTIVE DIRECTOR OR DELEGATE |
|
|
|
|
DATE |
||||||||||||||||||||
BURIALREQUEST - INVOICE |
COMMONWEALTH OF PENNSYLVANIA - DEPARTMENTOF PUBLIC WELFARE |
PA118 11/07 |
INVOICE TO:
COMMONWEALTH OF PENNSYLVANIA DEPARTMENTOF PUBLIC WELFARE
OFFICE OF INCOME MAINTENANCE
*TO BE COMPLETED BYFUNERALDIRECTOR
BURIAL/CREMATION CHARGES FOR
DECEASED
|
|
|
|
|
|
|
|
|
CEMETERYWHERE BURIED |
|
CITY |
|
|
DATE OF BURIAL |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
1.Maximum payment allowance requested from DPW for burial and/or cremation ($750.00 per deceased person).
2.Resources that reduce DPW payment
Resources applicable to cost of burial and/or cremation:
$
RESOURCE
AMOUNT
Resources that will reduce DPW payment |
TOTAL= |
3.Contributions that may reduce DPW payment from friends, relatives, other entities, i.e. Fraternal organizations, etc.
$
CONTRIBUTOR |
AMOUNT |
|
|
TOTALCONTRIBUTIONS
Excess = Total contributions minus $750.00 per deceased person.
4.Total resources and/or contributions (excess over $750.00 per deceased person) that will reduce DPW payment. If total is 0 or less, enter 0.
5.DPW payment owing after reduction for resources and/or contributions exceeding $750.00 per deceased person ($750.00 per deceased person, minus item 4).
6.Total DPW payment to funeral service provider (item 5 repeated).
$
$
$
$
$
CERTIFICATION OF FUNERALDIRECTOR
I certify that the amount listed in Item 5 constitutes the entire bill incidental to the burial/cremation of the person named above, that no payment has been, or will be, accepted from any other source, and that I will notify the CountyAssistance Office promptly of any additional resources that come to my attention. By signing, Icertify that I understand that the Department of Public Welfare can impose penalties such as reimbursement and prosecution for any violations of funeral payment regulations.
SIGNATURE OF FUNERALDIRECTOR |
|
DATE |
|
|
|
FIRM NAME AND ADDRESS
Provider MAID Number
Provider Address Code
PA118 11/07