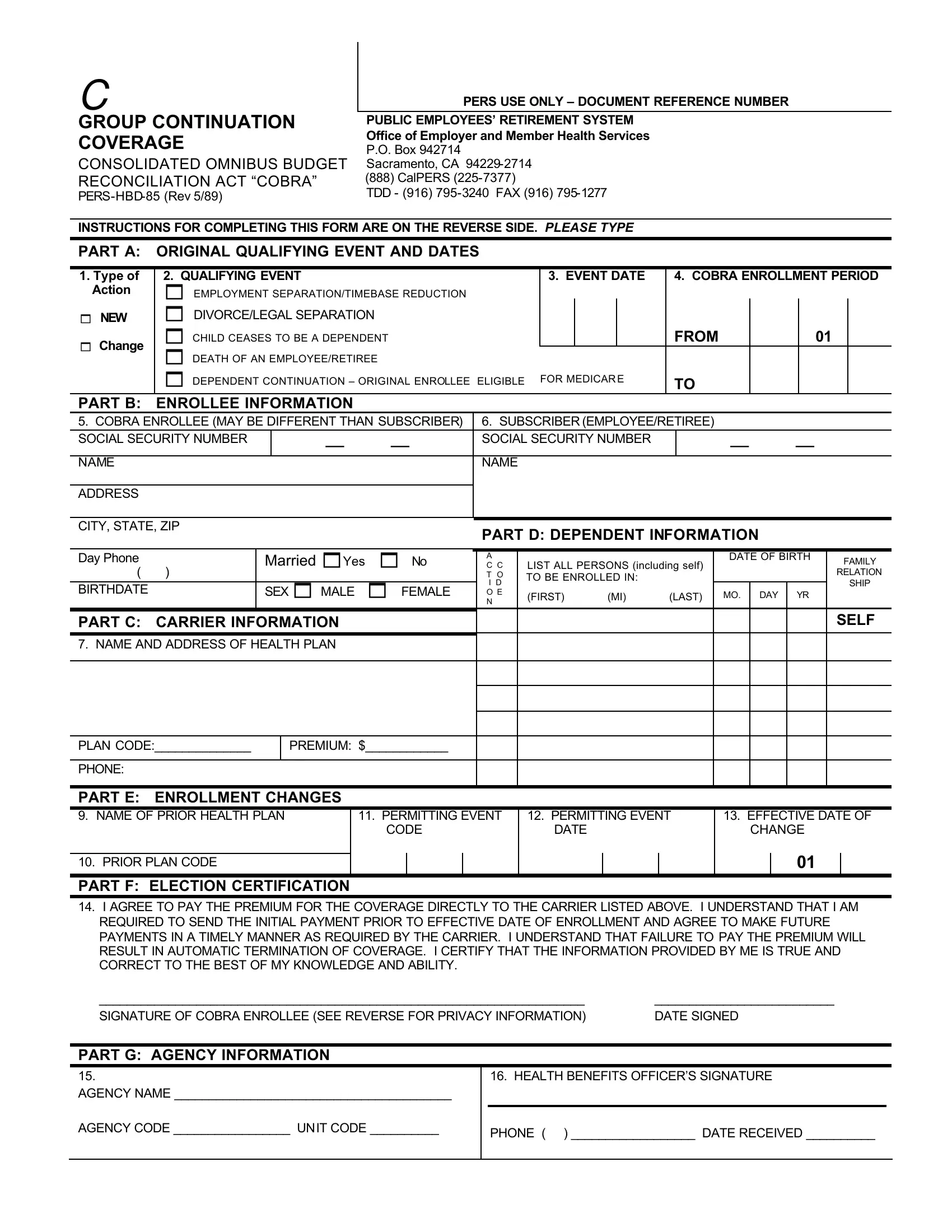
Understanding the intricacies of health benefits post-employment or after major life changes can be quite daunting. The Pers Hbd 85 form, also known as the Public Employees' Retirement System (PERS) COBRA Continuation Coverage application, plays a pivotal role in this arena by offering a crucial bridge for individuals navigating the complexities of maintaining health coverage during transitional periods. Designed under the auspices of the Consolidated Omnibus Budget Reconciliation Act (COBRA), this document facilitates the extension of health benefits previously provided by public employers to employees, retirees, and their dependents in California. In essence, the form allows eligible individuals to continue their health insurance coverage when it would otherwise be lost due to specific qualifying events such as employment separation, divorce, or the death of the employee/retiree. Detailing essential information such as enrollee details, event dates, and coverage information, the form also outlines procedural guidelines for applying, including the necessary steps for electing COBRA coverage, the payment to carriers, and the implications of non-compliance. The form is not just a piece of paperwork but a crucial lifeline that ensures continuity of care for those in a state of transition, emphasizing the importance of timely and accurate submission to avoid any interruption in coverage.
| Question | Answer |
|---|---|
| Form Name | Form Pers Hbd 85 |
| Form Length | 2 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 30 sec |
| Other names | TIMEBASE, PERS-HBD-85, pers hbd 85, 1977 |