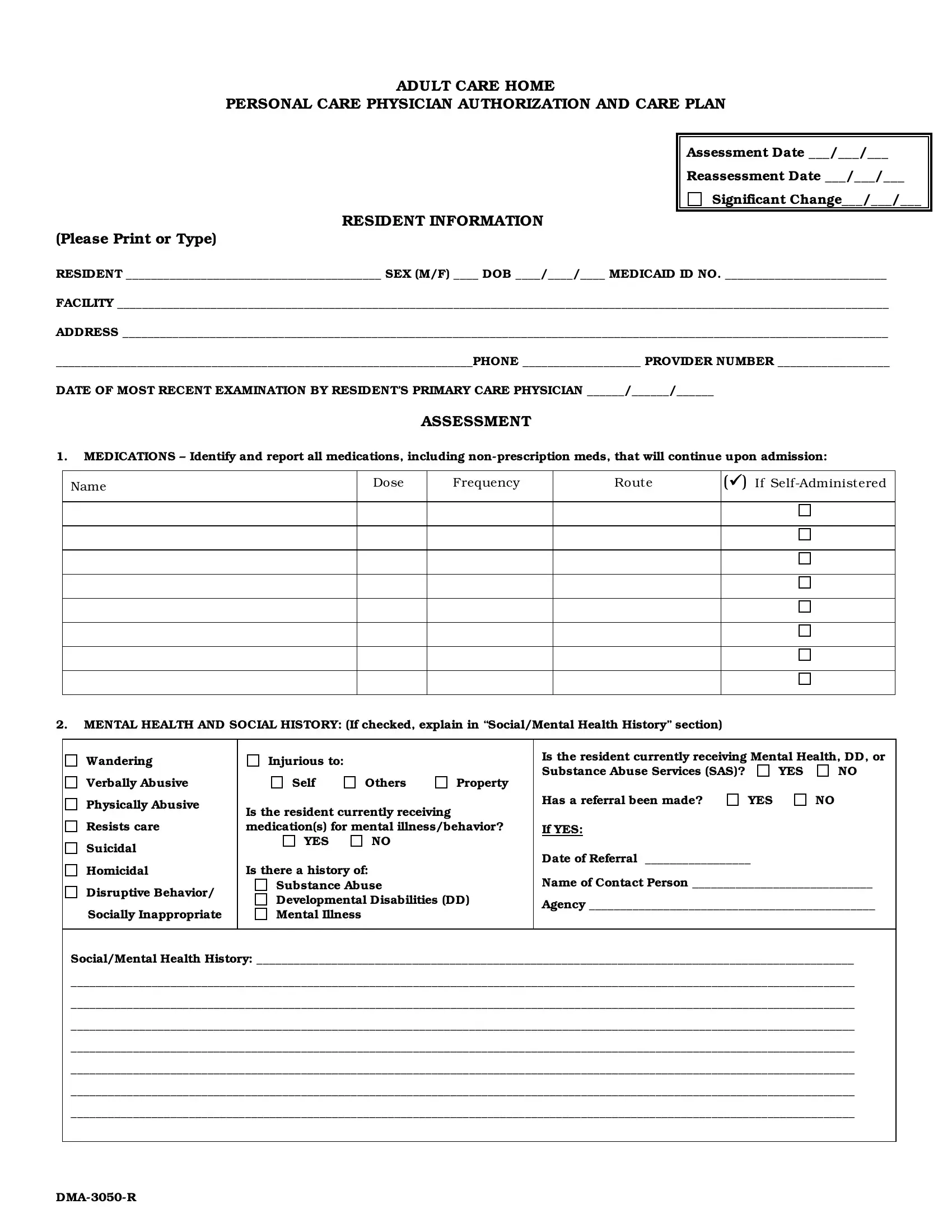
The Adult Care Home Personal Care Physician Authorization and Care Plan is a comprehensive document designed to ensure that residents of adult care homes receive the personalized care they need and deserve. At the core of this form is the resident's health assessment, which evaluates everything from medication needs, mental health and social history, to the finer points of daily living assistance requirements. These include mobility, nutrition intake, skin care, and more. Critical to the form is the need for detailed communication between the care facility and the resident's physician, ensuring that all medical diagnoses and the necessary personal care services are accurately documented and authorized. Besides medical aspects, the form also touches on important areas such as the resident's ability to perform daily living activities (ADLs), which covers eating, toileting, and grooming, among others. Each task is carefully assessed to determine the level of assistance required, demonstrating a thorough planning process aimed at providing tailored care. This process not only ensures the resident's health and safety but also respects their dignity and independence as much as possible. The ultimate goal is to create a supportive environment where residents can maintain the highest quality of life.
| Question | Answer |
|---|---|
| Form Name | Form Personal Care |
| Form Length | 5 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 1 min 15 sec |
| Other names | personal physician authorization, printable inservices for caregivers, care physician authorization, form personal care |