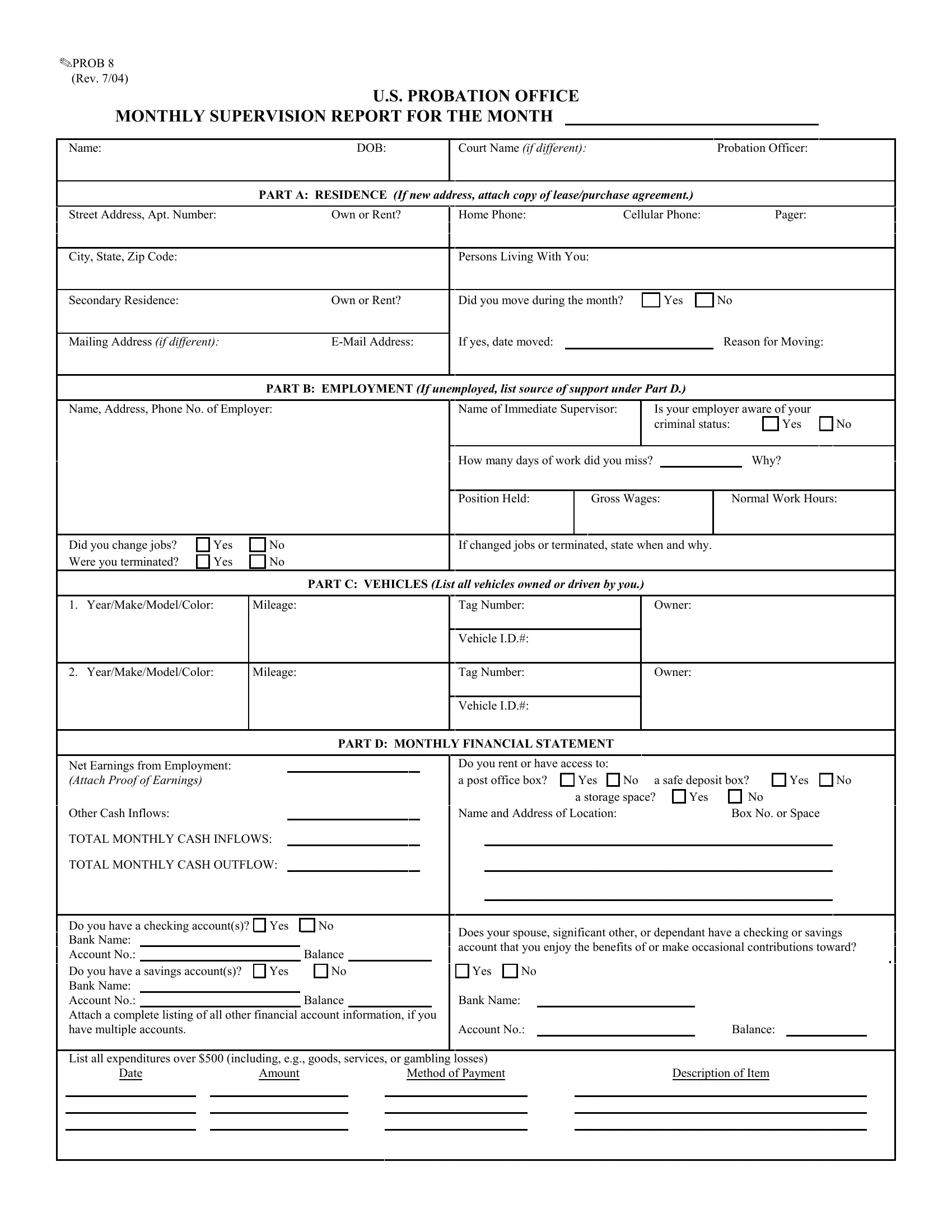
The Prob 8 form, revised in July 2004 and officially known as the U.S. Probation Office Monthly Supervision Report, serves a critical function in the federal probation system by keeping probation officers apprised of the monthly status of individuals under their supervision. It meticulously gathers detailed information across various aspects of a probationer’s life, including residence, employment or source of support if unemployed, vehicle ownership, financial standings, and compliance with supervision conditions. Consequently, the form requires probationers to report any changes in address, employment status, encounters with law enforcement, financial fluctuations, and more. Its structured sections—ranging from personal identification to detailed financial accounts—underscore the thorough monitoring process, aiming to ensure the individuals adhere to the terms of their probation and facilitate their reintegration into society. Furthermore, the form holds a stern warning about the severe consequences of submitting false information, highlighting the importance of transparency in the probation process. By mandating the submission of this report, the probation office underscores its commitment to closely monitoring individuals under its supervision, ensuring public safety, and assisting in the probationers' rehabilitation and reintegration efforts.
| Question | Answer |
|---|---|
| Form Name | Form Prob 8 |
| Form Length | 2 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 30 sec |
| Other names | monthly supervision, sample report of examination supervision, examination supervision report, supervisor report template |
OPROB 8 (Rev. 7/04)
U.S. PROBATION OFFICE
MONTHLY SUPERVISION REPORT FOR THE MONTH
Name:DOB:
Court Name (if different): |
Probation Officer: |
PART A: RESIDENCE (If new address, attach copy of lease/purchase agreement.)
Street Address, Apt. Number: |
Own or Rent? |
Home Phone: |
Cellular Phone: |
Pager: |
City, State, Zip Code:
Persons Living With You:
Secondary Residence: |
Own or Rent? |
Did you move during the month?
Yes
No
Mailing Address (if different): |
If yes, date moved: |
|
Reason for Moving: |
PART B: EMPLOYMENT (If unemployed, list source of support under Part D.)
Name, Address, Phone No. of Employer:
Name of Immediate Supervisor:
Is your employer aware of your
criminal status: |
|
Yes |
|
|
|
No
How many days of work did you miss? |
|
Why? |
Position Held:
Gross Wages:
Normal Work Hours:
Did you change jobs? |
Yes |
Were you terminated? |
Yes |
1. Year/Make/Model/Color:
|
No |
|
|
If changed jobs or terminated, state when and why. |
||
|
No |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
PART C: VEHICLES (List all vehicles owned or driven by you.) |
|
|||
|
|
|
|
|
|
|
Mileage: |
|
|
Tag Number: |
|
Owner: |
|
Vehicle I.D.#:
2. Year/Make/Model/Color:
Mileage:
Tag Number:
Vehicle I.D.#:
Owner:
Net Earnings from Employment: (Attach Proof of Earnings)
Other Cash Inflows:
TOTAL MONTHLY CASH INFLOWS:
TOTAL MONTHLY CASH OUTFLOW:
PART D: MONTHLY FINANCIAL STATEMENT
Do you rent or have access to: |
|
|
|
|
||
a post office box? |
Yes |
No a safe deposit box? |
Yes |
|||
|
|
a storage space? |
Yes |
No |
|
|
Name and Address of Location: |
|
|
Box No. or Space |
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
No
Do you have a checking account(s)? |
Yes |
No |
|
Bank Name: |
|
|
|
Account No.: |
|
|
Balance |
Do you have a savings account(s)? |
Yes |
No |
|
Bank Name: |
|
|
|
Account No.: |
|
|
Balance |
Attach a complete listing of all other financial account information, if you have multiple accounts.
Does your spouse, significant other, or dependant have a checking or savings account that you enjoy the benefits of or make occasional contributions toward?
Yes No
Bank Name:
Account No.: |
|
Balance: |
List all expenditures over $500 (including, e.g., goods, services, or gambling losses) |
|
||
Date |
Amount |
Method of Payment |
Description of Item |
OPROB 8 |
Page 2 |
(Rev. 7/04) |
|
|
|
|
PART E: COMPLIANCE WITH CONDITIONS OF SUPERVISION DURING THE PAST MONTH |
Were you questioned by any law enforcement officers?
Yes |
No |
Were you arrested or named as a defendant in any criminal case?
Yes |
No |
If yes, date:
If yes, when and where?
Agency:
Charges:
Reason:
Disposition:
(Attach copy of citation, receipt, charges, disposition, etc.)
Were any pending charges disposed of during the month?
Yes |
No |
If yes, date:
Court:
Disposition:
Did you have any contact with anyone having a criminal record?
Yes |
No |
If yes, whom?
Was anyone in your household arrested or questioned by law enforcement?
|
|
|
Yes |
No |
If yes, whom? |
|
|
||
Reason: |
|
|
||
Disposition: |
|
|
||
|
|
|||
Did you possess or have access to a firearm? |
|
|||
|
|
|
Yes |
No |
If yes, why? |
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Did you possess or use any illegal drugs? |
|
|
|
|
|
|
|
Did you travel outside the district without permission? |
|
||||||||||||
|
|
|
|
|
Yes |
|
No |
|
|
|
|
|
|
|
|
|
Yes |
No |
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
If yes, type of drug: |
|
|
|
|
|
|
|
|
If yes, when and where? |
|
|
|
|||||||||
|
|
|
|
|
|
|
|
|
|||||||||||||
|
|
|
|
|
|
|
|
|
|||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
Do you have a special assessment, restitution, or fine? |
Yes |
No |
If yes, amount paid during the month: |
|
|
||||||||||||||||
Special Assessment: |
|
|
|
Restitution: |
|
|
|
|
|
|
|
|
Fine: |
|
|
|
|||||
NOTE: ALL PAYMENTS TO BE MADE BY MONEY ORDER (POSTAL OR BANK) OR CASHIER’S CHECK ONLY.
Do you have community service work to perform?
Yes |
No |
Number of hours completed this month:
Do you have drug, alcohol, or mental health aftercare?
Yes |
No |
If yes, did you miss any sessions during this month?
Yes |
No |
Number of hours missed:
Balance of hours remaining:
WARNING: ANY FALSE STATEMENTS MAY RESULT IN REVOCATION OF PROBATION, SUPERVISED RELEASE, OR PAROLE, IN ADDITION TO 5 YEARS IMPRISONMENT, A $250,000
FINE, OR BOTH.
(18 U.S.C. § 1001)
Did you fail to respond to phone recorder instructions?
Yes |
No |
If yes, why?
I CERTIFY THAT ALL INFORMATION FURNISHED IS COMPLETE
AND CORRECT.
SIGNATURE |
DATE |
REMARKS:
RECEIVED:
MailOC
HCCC
RETURN TO:
U.S. Probation Officer |
Date |
|
|