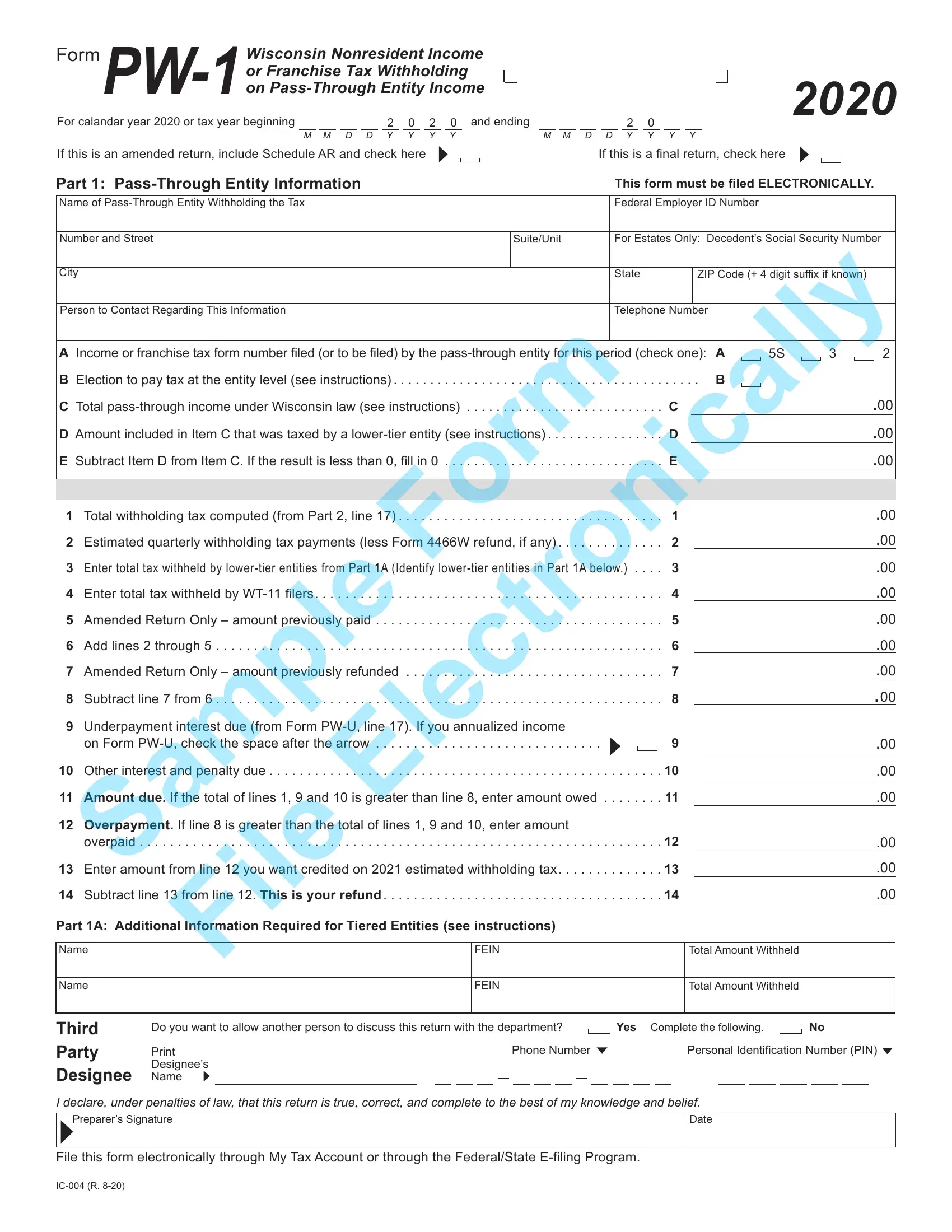
Pension Wise is a government-backed scheme aimed at helping people understand their retirement options and make the most of their savings. The scheme offers free, impartial guidance to anyone over 50 years old who is thinking about how to best use their pensions. In this blog post, we will take a closer look at Form Pw 1 – what it is, what you need to do to complete it, and the benefits of using Pension Wise’s services.
| Question | Answer |
|---|---|
| Form Name | Form Pw 1 |
| Form Length | 2 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 30 sec |
| Other names | wisconsin pw 1 form, wi income through, wisconsin pw 1, wi pw 1 extension |

For calandar year 2020 or tax year beginning |
|
|
|
|
|
|
|
|
2 0 2 0 and ending |
2 0 |
|
|
|
|
|||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
M M D D Y Y Y Y |
M M D D Y Y Y Y |
|||||||||||||||||||||||||||||
2020
If this is an amended return, include Schedule AR and check here If this is a final return, check here
Part 1: |
|
|
|
This form must be filed ELECTRONICALLY. |
|||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
||||||
Name of |
|
|
|
|
Federal Employer ID Number |
|
|
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
||||||
Number and Street |
|
|
|
Suite/Unit |
|
For Estates Only: Decedent’s Social Security Number |
|||||||||||
|
|
|
Electronically |
|
|
||||||||||||
City |
|
|
|
|
|
|
State |
|
|
ZIP Code (+ 4 digit suffix if known) |
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
Person to Contact Regarding This Information |
|
|
|
|
Telephone Number |
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Form |
|
|
|
|
|
|
|
|
|
|
|
||
A Income or franchise tax form number filed (or to be filed) by the |
A |
5S |
3 |
2 |
|
||||||||||||
B Election to pay tax at the entity level (see instructions) |
. . . . . . . . . |
B |
|
|
|||||||||||||
C Total |
. . . . |
. |
C. . . . |
. . . . |
|
|
.00 |
|
|||||||||
D Amount included in Item C that was taxed by a |
. . . . |
|
. D. . . . |
. |
|
|
|
.00 |
|
||||||||
E Subtract Item D from Item C. If the result is less than 0, fill in 0 |
. . . . . |
|
. E. . . . |
. . . . |
|
|
.00 |
|
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
1 |
Total withholding tax computed (from Part 2, line 17) |
. . . . . . . . . . . . . . . . . . |
. . . . . . . . . . . . . . . |
|
. . |
|
|
1 |
|
|
|
|
|
.00 |
|||
2 |
Estimated quarterly withholding tax payments (less orm 4466W refund, if any) |
. . . . . |
|
|
2 |
|
|
|
|
|
.00 |
||||||
3 |
Sample |
|
|
|
w.) . . . |
. |
3 |
|
|
|
|
|
.00 |
||||
Enter total tax withheld by |
|
|
|
|
|
||||||||||||
4 |
. . . . . . .Enter total tax withheld by |
. . . . . . . . . . |
. . . . . . . . . . . . . . . . . . . . . . . |
. . . . . . |
|
|
|
|
4 |
|
|
|
|
|
.00 |
||
5 |
Amended Return Only – amount previous y paid . . . |
. . . . . . . . . . . . . . . |
. . . . . . . . . . . . |
. . . . |
. . . |
. 5 |
|
|
|
|
|
.00 |
|||||
6 |
Add lines 2 through 5 |
. . . . . . . . . |
. . . . . . . |
. . . . . . . . . . . . . . |
. . . . . . . . . . . . . |
|
. . . . . . |
. |
. 6 |
|
|
|
|
|
.00 |
||
7 |
Amended Return Only – amount |
reviously refunded |
. 7 |
|
|
|
|
|
.00 |
||||||||
8 |
Subtract line 7 from 6 |
. . . . . . . . . |
. . . . . . . . . . . . . . . . . . . . . . . |
. . . . . . . . . . . . . . |
|
. . . . |
|
|
8 |
|
|
|
|
|
.00 |
||
9 |
Underpayment interest due (from Form |
|
|
|
|
|
|
|
|
|
|
|
|||||
|
on Form |
. . . . . . . . . . . . . . . |
. . . . . . . . . . . . |
|
|
|
|
9 |
|
|
|
|
|
.00 |
|||
10 |
Other interest nd penalty due . |
. . . . . . . . . . |
. . . . . . . |
. . . . . . . . . . . . . . . . |
. . . . . . . . . . . . . |
. |
. . . |
. |
|
10 |
|
|
|
|
|
.00 |
|
11 |
Amount due. If the total of lines 1, 9 and 10 is greater than line 8, enter amount owed . |
. . . . . . |
. |
11 |
|
|
|
|
|
.00 |
|||||||
12 |
Overpayment. If line 8 is gr at |
r than the total of lines 1, 9 and 10, enter amount |
|
|
|
|
|
|
|
|
|
|
|
||||
|
overpaid |
. . . . . . . . . |
. . . . . . . . . . . . . . . . . . . . . |
. . . . . . . . . . . . . |
|
. . . |
. . . |
. |
12. |
|
|
|
|
|
.00 |
||
13 |
Enter amount from line 12 you want cr dit d on 2021 estimated withholding tax |
|
|
13 |
|
|
|
|
|
.00 |
|||||||
14 |
Subtract line 13 from l ne 12 . Th s is your refund. . . |
. . . . . . . . . . . . . . . . . . . . |
. . . . . . . . . . . . . . |
|
|
|
|
14 |
|
|
|
|
|
.00 |
|||
Part 1A: Additional Information Required for Tiered Entities (see instructions)
Name |
File |
FEIN |
Total Amount Withheld |
|
|
|
|
Name |
|
FEIN |
|
|
|
|
|
Third
Party
Designee
Do you want to allow another person to discuss this return with the department? |
|
|
Yes Complete the following . |
|
|
No |
||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
Phone Number |
|
|
|
|
|
|
Personal Identification Number (PIN) |
||||||||||||||||||||||||
Designee’s |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
Name |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
I declare, under penalties of law, that this return is true, correct, and complete to the best of my knowledge and belief.
Preparer’s Signature
Date
File this form electronically through My Tax Account or through the Federal/State
2020 Form |
|
|
|
|
|
|
|
|
|
|
|
Page 2 of 2 |
||||
Part 2: Nonresident Shareholder, Partner, Member, or Beneficiary Information |
|
|
|
|
|
|||||||||||
(Note: See instructions corresponding to each column letter) |
|
|
|
|
|
If affidavit (Form |
||||||||||
|
|
|
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
h |
Address |
|
|
SSN |
|
|
|
|
Electronically$$ |
$ |
|
$ |
|
|||
|
|
A . |
|
B . |
C . |
|
D . |
|
E . |
F. |
G . |
|
H . |
|
||
L |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
i |
|
|
|
|
|
|
|
|
|
|
Share of |
|
|
|
|
|
n |
|
|
|
|
|
|
Affidavit |
|
Wisconsin |
|
|
|
Withholding |
|
||
e |
|
|
|
|
|
Tax |
|
Taxable |
Gross |
Share of |
|
Tax |
|
|||
|
|
|
|
|
|
|
Form |
|
Tax Credits |
|
Computed |
|
||||
|
|
Nonresident’s Name and Address |
|
FEIN or SSN |
Form |
|
Filed |
|
Income |
Withholding |
|
|
||||
|
Name |
|
|
FEIN |
|
|
|
Yes |
|
|
|
|
|
|
|
|
a |
Address |
|
|
SSN |
|
|
|
No |
$ |
$ |
$ |
|
$ |
|
||
|
Name |
|
|
FEIN |
|
|
|
|
|
|
|
|
|
|
|
|
b |
|
|
|
|
|
|
|
|
Yes |
$ |
$ |
$ |
|
$ |
|
|
Address |
|
|
SSN |
|
|
|
No |
|
|
|||||||
|
Name |
|
|
FEIN |
|
|
|
Yes |
|
|
|
|
|
|
|
|
c |
Address |
|
|
SSN |
|
|
|
No |
$ |
$ |
$ |
|
$ |
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
i |
Name |
Sample |
|
|
|
Yes |
$ |
$ |
$ |
|
$ |
|
||||
|
|
|
FEIN |
|
|
|
Yes |
|
|
|
|
|
|
|
||
d |
Address |
|
|
SSN |
|
|
|
No |
$ |
$ |
$ |
|
$ |
|
||
|
Name |
|
|
FEIN |
|
|
|
Yes |
|
|
|
|
|
|
|
|
e |
Address |
|
|
SSN |
|
|
|
No |
$ |
$ |
$ |
|
$ |
|
||
|
Name |
|
|
FEIN |
|
|
|
Y s |
|
|
|
|
|
|
|
|
f |
Address |
|
|
SSN |
|
|
|
No |
$ |
$ |
$ |
|
$ |
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Name |
|
|
FEIN |
|
|
|
Yes |
|
|
|
|
|
|
|
|
g |
|
|
|
|
|
|
|
|
$ |
$ |
$ |
|
$ |
|
||
|
|
|
|
|
|
|
|
|
|
|
||||||
Address |
|
|
SSN |
|
|
|
No |
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Name |
File |
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
FEIN |
|
|
|
Yes |
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
No |
|
|
|
|
|
|
|
|
Name |
|
|
FEIN |
|
|
|
|
|
|
|
|
|
|
|
|
|
Address |
|
|
SSN |
|
|
|
No |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Total Wisconsin income (add lines a through i) |
. . . |
|
|
|
|
|
|||||||||
|
|
|
|
|
|
|
|
|
|
$ |
|
|
|
|
|
|
|
15 Total withholding this page |
. . . . . . . . . . . . . |
. . . . . . |
|||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
$ |
|
|
16 Number of additional pages included |
|
. Total of line 15 amount from all additional pages |
. |
$ |
|
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
17 Total withholding tax computed . Add lines 15 and 16 . Enter total on Part 1, line 1 |
|
.$ |
|
||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|