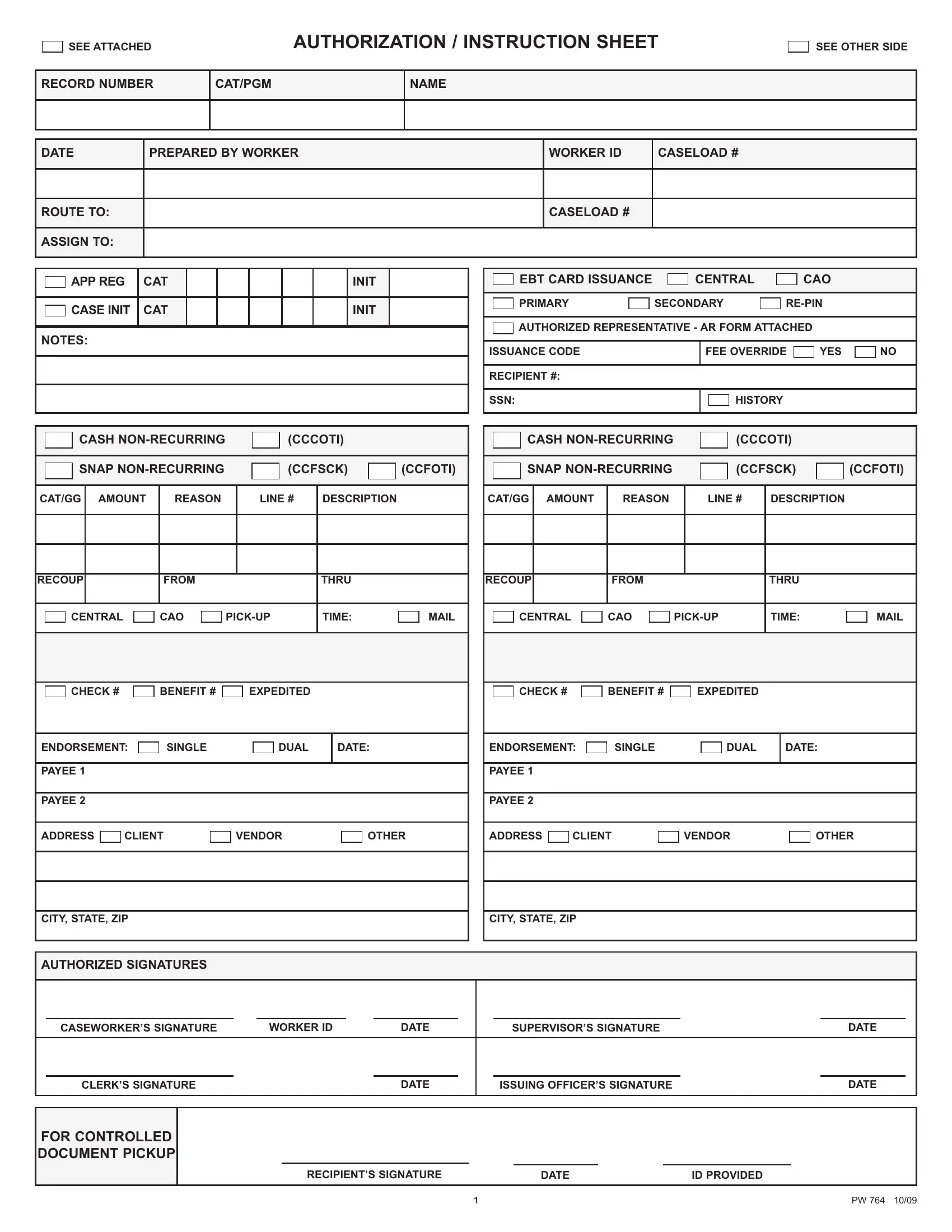
Understanding the PW 764 form is essential for anyone navigating a range of assistance programs. This comprehensive document is designed to streamline the process of requesting and issuing benefits across various categories. It encompasses everything from cash assistance and Supplemental Nutrition Assistance Program (SNAP) benefits to other non-recurring aids. The form is utilized by case workers to record critical information, such as the preparation details, caseload numbers, and routing instructions, to ensure the prompt and accurate distribution of aid. With sections that detail amounts, reasons, recipient information, payment processing (including checks and Electronic Benefit Transfer (EBT) card issuance), and authorized signatures, the PW 764 form lays the groundwork for transparent and efficient benefit administration. This document not only facilitates the management of recurring and non-recurring benefits but also includes provisions for special circumstances such as expedited service and controlled document pickup. Additionally, it plays a role in managing case specifics, including data verification, marital status, and more, which are crucial for tailoring assistance to individual needs. Thus, the PW 764 form is a vital tool in the administration of assistance programs, ensuring that support reaches those who need it in a timely and organized manner.
| Question | Answer |
|---|---|
| Form Name | Form Pw 764 |
| Form Length | 2 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 30 sec |
| Other names | pw 764, pw764, HIB, MARIT |
SEE ATTACHED
AUTHORIZATION / INSTRUCTION SHEET
SEE OTHER SIDE
RECORD NUMBER |
CAT/PGM |
NAME |
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
DATE |
PREPARED BYWORKER |
|
WORKER ID |
CASELOAD # |
|
|
|
|
|
|
|
|
|
|
|
|
|
ROUTE TO: |
|
|
|
CASELOAD # |
|
|
|
|
|
|
|
ASSIGN TO: |
|
|
|
|
|
|
|
|
|
|
|
|
|
APPREG |
|
CAT |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
INIT |
|
|
|
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
CASEINIT |
|
CAT |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
INIT |
|
|
|
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
NOTES: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
|
|
CASH |
|
|
|
|
|
|
(CCCOTI) |
|
|
||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
(CCFSCK) |
|
(CCFOTI) |
|||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
CAT/GG |
|
AMOUNT |
REASON |
|
|
|
|
LINE # |
|
DESCRIPTION |
|
|
||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
RECOUP |
|
|
|
|
|
|
|
|
FROM |
|
|
|
|
|
|
|
|
THRU |
|
|
||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
CENTRAL |
|
|
|
|
CAO |
|
|
|
|
TIME: |
|
|||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
CHECK # |
|
|
|
|
BENEFIT # |
|
|
|
|
|
EXPEDITED |
|
|
|
|
|
|
|
|
|
|
|||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||
ENDORSEMENT: |
|
|
SINGLE |
|
|
|
|
|
DUAL |
|
|
DATE: |
|
|
||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
PAYEE 1 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
PAYEE 2 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
ADDRESS |
|
CLIENT |
|
|
|
VENDOR |
|
|
|
|
|
OTHER |
||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||||
CITY, STATE, ZIP
|
|
EBT CARD ISSUANCE |
|
|
CENTRAL |
|
|
CAO |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
PRIMARY |
SECONDARY |
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
AUTHORIZED REPRESENTATIVE - AR FORM ATTACHED |
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
ISSUANCE CODE |
|
|
|
FEE OVERRIDE |
YES |
NO |
||||
|
|
|
|
|
|
|
|
|
|
|
RECIPIENT #: |
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
SSN: |
|
|
|
HISTORY |
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
CASH |
|
|
|
|
|
|
(CCCOTI) |
|
|
||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
(CCFSCK) |
|
(CCFOTI) |
|||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
CAT/GG |
|
AMOUNT |
REASON |
|
|
|
|
LINE # |
DESCRIPTION |
|
|
|||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
RECOUP |
|
|
|
|
|
|
|
FROM |
|
|
|
|
|
|
|
THRU |
|
|
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
CENTRAL |
|
|
|
CAO |
|
|
|
TIME: |
|
|||||||||||||||||
|
|
|
|
|
|
|
|
|
||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
CHECK # |
|
|
|
BENEFIT # |
|
|
|
|
EXPEDITED |
|
|
|
|
|
|
|
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
ENDORSEMENT: |
|
|
SINGLE |
|
|
|
|
|
DUAL |
|
DATE: |
|
|
|||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
PAYEE 1 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
PAYEE 2 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
ADDRESS |
|
CLIENT |
|
|
|
|
VENDOR |
|
|
|
OTHER |
|||||||||||||||||
|
|
|
|
|
|
|
|
|||||||||||||||||||||
CITY, STATE, ZIP
AUTHORIZED SIGNATURES
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
CASEWORKER’S SIGNATURE |
WORKER ID |
|
DATE |
|
SUPERVISOR’S SIGNATURE |
|
|
DATE |
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
CLERK’S SIGNATURE |
|
|
|
DATE |
|
ISSUING OFFICER’S SIGNATURE |
|
|
DATE |
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
FOR CONTROLLED |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
DOCUMENT PICKUP |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
RECIPIENT’S SIGNATURE |
|
|
DATE |
ID PROVIDED |
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
1 |
PW 764 10/09 |