Form Ri Eft 1 is a form that must be completed and filed in order to create a valid Rhode Islandreal estate contract. The form can be used for both residential and commercial property transactions, and it is important that you complete it accurately to avoid any legal issues down the road. In this blog post, we will go over the basics of Form Ri Eft 1 so that you can understand what is required of you when completing it. We will also provide a few tips on how to make the process smoother for both you and the other party involved in the transaction. Thanks for reading!
| Question | Answer |
|---|---|
| Form Name | Form Ri Eft 1 |
| Form Length | 2 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 30 sec |
| Other names | EFT1 authorization agreement to the ri division of taxation eft section rhode island form |
FORM |
STATE OF RHODE ISLAND |
||||||
|
|
|
DEPARTMENT OF REVENUE |
||||
|
|
|
DIVISION OF TAXATION |
||||
|
|
|
ONE CAPITOL HILL |
||||
|
|
|
PROVIDENCE, RI |
||||
|
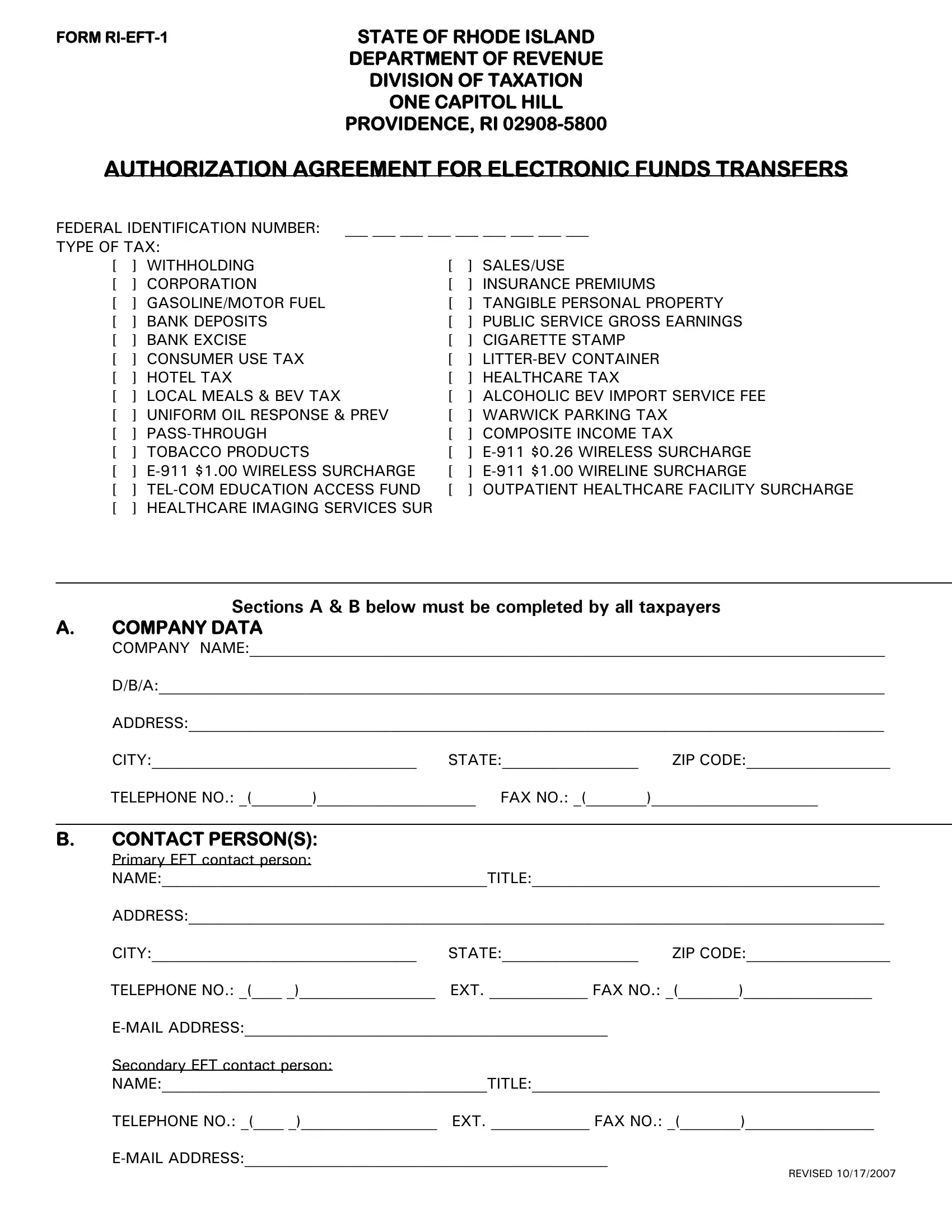
AUTHORIZATION AGREEMENT FOR ELECTRONIC FUNDS TRANSFERS |
|
|||||
FEDERAL IDENTIFICATION NUMBER: |
___ ___ ___ ___ ___ ___ ___ ___ ___ |
|
|||||
TYPE OF TAX: |
|
|
|
|
|
||
[ |
] WITHHOLDING |
|
[ |
] SALES/USE |
|||
[ |
] CORPORATION |
|
[ |
] INSURANCE PREMIUMS |
|||
[ |
] GASOLINE/MOTOR FUEL |
|
[ |
] TANGIBLE PERSONAL PROPERTY |
|||
[ |
] BANK DEPOSITS |
|
[ |
] PUBLIC SERVICE GROSS EARNINGS |
|||
[ |
] BANK EXCISE |
|
[ |
] CIGARETTE STAMP |
|||
[ |
] CONSUMER USE TAX |
|
[ |
] |
|||
[ |
] HOTEL TAX |
|
[ |
] HEALTHCARE TAX |
|||
[ |
] LOCAL MEALS & BEV TAX |
|
[ |
] ALCOHOLIC BEV IMPORT SERVICE FEE |
|||
[ |
] UNIFORM OIL RESPONSE & PREV |
[ |
] WARWICK PARKING TAX |
||||
[ |
] |
|
[ |
] COMPOSITE INCOME TAX |
|||
[ |
] TOBACCO PRODUCTS |
|
[ |
] |
$0.26 WIRELESS SURCHARGE |
||
[ |
] |
[ |
] |
$1.00 WIRELINE SURCHARGE |
|||
[ |
] |
[ |
] OUTPATIENT HEALTHCARE FACILITY SURCHARGE |
||||
[ |
] HEALTHCARE IMAGING SERVICES SUR |
|
|
|
|
||
Sections A & B below must be completed by all taxpayers
A.COMPANY DATA
COMPANY NAME:____________________________________________________________________________________
D/B/A:________________________________________________________________________________________________
ADDRESS:____________________________________________________________________________________________
CITY:___________________________________ STATE:__________________ ZIP CODE:___________________
TELEPHONE NO.: _(________)_____________________ FAX NO.: _(________)______________________
B.CONTACT PERSON(S):
Primary EFT contact person:
NAME:___________________________________________TITLE:______________________________________________
ADDRESS:____________________________________________________________________________________________
CITY:___________________________________ |
STATE:__________________ |
ZIP CODE:___________________ |
TELEPHONE NO.: _(____ _)__________________ |
EXT. _____________ FAX NO.: _(________)_________________ |
|
Secondary EFT contact person:
NAME:___________________________________________TITLE:______________________________________________
TELEPHONE NO.: _(____ _)__________________ EXT. _____________ FAX NO.: _(________)_________________
REVISED 10/17/2007
FORM
CHOOSE ONLY ONE OF THE TWO PAYMENT OPTIONS BELOW
C.ACH DEBIT OPTION
This section is to be completed only if you choose the ACH DEBIT OPTION.
TWO DEBIT OPTIONS AVAILABLE:
1.INTERNET FILING: Simply log onto https://www.ri.gov/taxation/business/index.php and click on the first time
user link. This is the only EFT registration process that you need to do.
Do not complete or remit this form to the RI Division of Taxation EFT Section.
2.TELEPHONE: Complete Section C and remit authorization agreement to the RI Division of Taxation EFT Section.
If ACH Debit is chosen, you authorize the Rhode Island Division of Taxation to present debit entries to your bank for the tax identified on the front. Only you can initiate a debit by calling the state's service bureau and indicating the amount of tax to be paid by electronic funds transfer.
Enclose a copy of a voided check or have an AUTHORIZED REPRESENTATIVE of your bank complete and sign this section of the form.
BANK NAME:_________________________________________________________________________________________
ADDRESS:____________________________________________________________________________________________
CITY:___________________________________ STATE:__________________ |
ZIP CODE:___________________ |
||||
BANK ACCOUNT #:______________________________ BANK ROUTING/TRANSIT |
NUMBER _______________________ |
||||
[ ] |
CHECKING |
[ ] |
SAVINGS |
|
|
____________________________________________________ |
____________________________________ |
||||
|
Printed Name of Bank Representative |
|
Telephone No. |
||
____________________________________________________ |
____________________________________ |
||||
|
Signature of Bank Representative |
|
Date |
||
D. ACH CREDIT OPTION
This section is to be completed only if you choose the ACH CREDIT OPTION.
All ACH CREDIT must be initiated in the required CCD+ and TXP format. Any payments not received in that format may be considered late.
Example:
Generic TXP addendum record CCD format
FIELD #: |
FIELD NAME: DATA ELEMENT TYPE: |
FIELD LENGTH: |
COMMENTS: |
|
|
Segment Id |
|
|
TXP |
|
Field Separator |
|
|
* |
TXP01 |
Taxpayer Id |
AN |
11 |
12345678900 |
|
Field Separator |
|
|
* |
TXP02 |
Tax Type Code |
ID |
5 |
55555 |
|
Field Separator |
|
|
* |
TXP03 |
Tax period End Date |
DT |
6 |
YYMMDD |
|
Field Separator |
|
|
* |
TXP04 |
Amount Type |
ID |
1 |
T(Tax) |
|
Field Separator |
|
|
* |
TXP05 |
Amount Paid |
N2 |
1/10 |
$$$$$$$$cc |
|
Record Terminator |
|
|
/ |
This form must be completed and mailed to: Electronic Funds Transfer Program
Rhode Island Division of Taxation
One Capitol Hill
Providence, RI
Phone (401)
FAX (401)
REVISED 10/17/2007