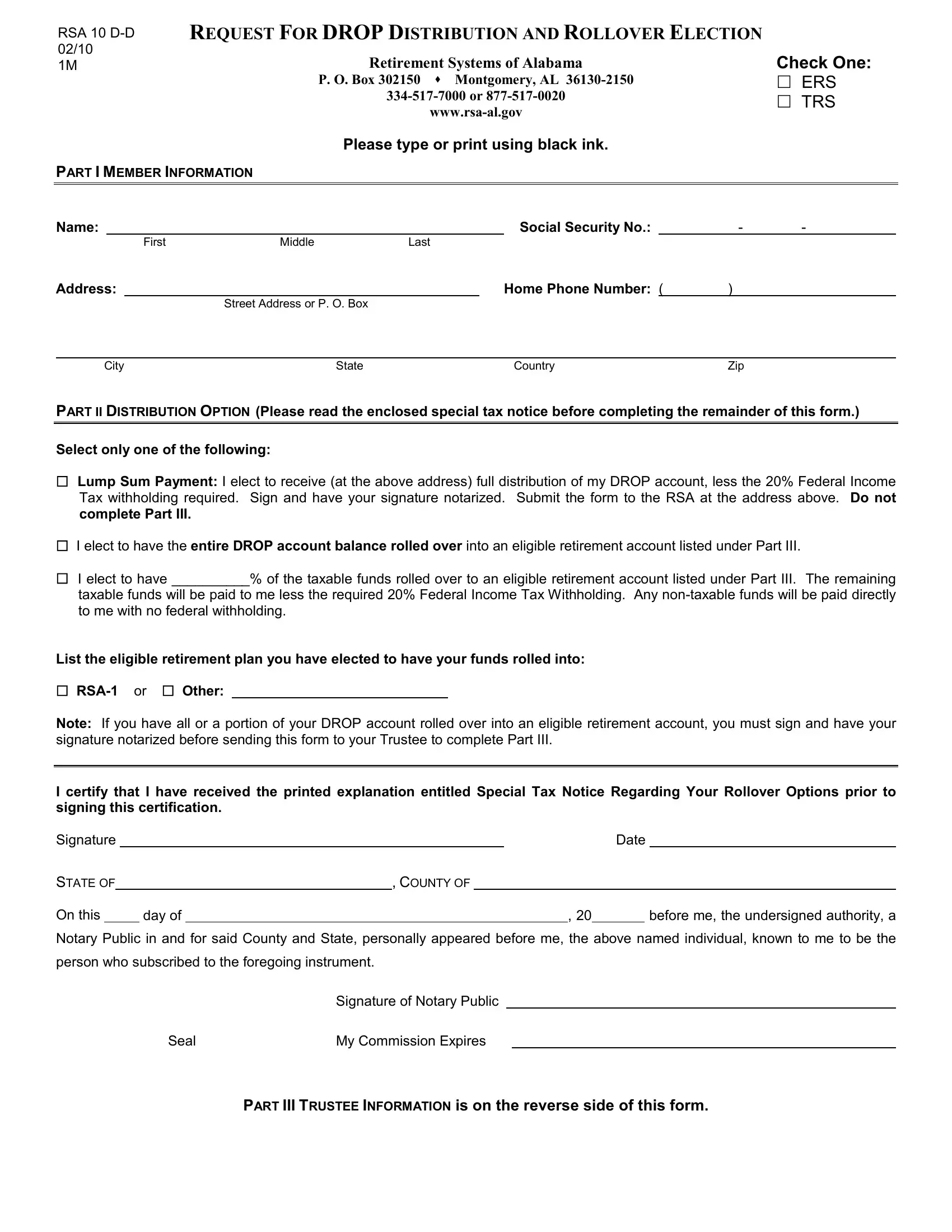
Understanding the RSA 10 D-D form is essential for members of the Retirement Systems of Alabama who are considering options regarding the distribution and rollover of their Deferred Retirement Option Plan (DROP) accounts. This comprehensive form, designed for clear communication between the member and the Retirement Systems of Alabama, must be completed with care and attention to detail, using black ink. Members are presented with critical choices, including receiving a lump sum payment subject to federal income tax withholding or electing a rollover to an eligible retirement account, which might offer tax advantages or deferments. The form is meticulous in its requirement for member information, distribution selections, and, if applicable, details about the chosen retirement account for the rollover, necessitating the endorsement of both the member and a notary. Moreover, it's crucial for members to acknowledge the receipt of the Special Tax Notice regarding rollover options, underscoring the importance of informed decision-making in the context of retirement planning. With spaces for the acknowledgment of non-taxable funds and the signature of the trustee accepting the rollover, the RSA 10 D-D form encapsulates a vital part of the retirement process, blending the need for precise personal details with the broader regulations governing retirement distributions and rollovers in the United States.
| Question | Answer |
|---|---|
| Form Name | Form Rsa 10 D D |
| Form Length | 2 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 30 sec |
| Other names | Request for DROP Distribution and Rollover Election rsa alabama retirement form |
RSA 10 |
REQUEST FOR DROP DISTRIBUTION AND ROLLOVER ELECTION |
|
02/10 |
|
Check One: |
1M |
Retirement Systems of Alabama |
|
|
P. O. Box 302150 Montgomery, AL |
ERS |
|
TRS |
|
|
||
|
|
Please type or print using black ink.
PART I MEMBER INFORMATION
Name: |
|
|
|
|
Social Security No.: |
|
- |
- |
|
|
|
First |
Middle |
Last |
|
|
|||
Address: |
|
|
|
Home Phone Number: ( |
) |
|
|||
|
|
|
Street Address or P. O. Box |
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
City |
State |
|
|
Country |
Zip |
|
|||
PART II DISTRIBUTION OPTION (Please read the enclosed special tax notice before completing the remainder of this form.)
Select only one of the following:
Lump Sum Payment: I elect to receive (at the above address) full distribution of my DROP account, less the 20% Federal Income Tax withholding required. Sign and have your signature notarized. Submit the form to the RSA at the address above. Do not complete Part III.
I elect to have the entire DROP account balance rolled over into an eligible retirement account listed under Part III.
I elect to have __________% of the taxable funds rolled over to an eligible retirement account listed under Part III. The remaining taxable funds will be paid to me less the required 20% Federal Income Tax Withholding. Any
List the eligible retirement plan you have elected to have your funds rolled into:
Note: If you have all or a portion of your DROP account rolled over into an eligible retirement account, you must sign and have your signature notarized before sending this form to your Trustee to complete Part III.
I certify that I have received the printed explanation entitled Special Tax Notice Regarding Your Rollover Options prior to signing this certification.
Signature |
|
|
|
|
|
|
|
|
Date |
|
|||
STATE OF |
|
|
|
, COUNTY OF |
|
|
|
||||||
On this |
|
|
|
day of |
|
|
|
, 20 |
|
before me, the undersigned authority, a |
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Notary Public in and for said County and State, personally appeared before me, the above named individual, known to me to be the person who subscribed to the foregoing instrument.
|
Signature of Notary Public |
Seal |
My Commission Expires |
PART III TRUSTEE INFORMATION is on the reverse side of this form.

PART III TRUSTEE INFORMATION (To be completed by Trustee receiving the rollover)
Member Name: |
|
|
|
Social Security No.: |
|
- |
- |
|||||
|
|
|
|
First |
Middle |
Last |
|
|
|
|
|
|
Trustee Name: |
|
|
|
|
Account Number: |
|
|
|||||
Contact Person: |
|
|
|
|
Phone No.: ( |
) |
|
|||||
Address: |
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
Street Address or P. O. Box |
|
City |
State |
|
Zip |
|||
Plan accepts
Plan does not accept
Type of account into which money will be rolled over:
401 Qualified Retirement Plan |
403(a) Annuity Contracts |
403(b) Tax Sheltered Annuity |
408(a) Individual Retirement Account 408(b) Individual Retirement Annuity Governmental Deferred Compensation
Roth IRA |
Compensation Plans (IRC 457) |
An Education IRA is not an eligible plan.
Signature of Trustee Official |
|
Date: |
Please submit the completed form to the RSA at the address on the front of this form.