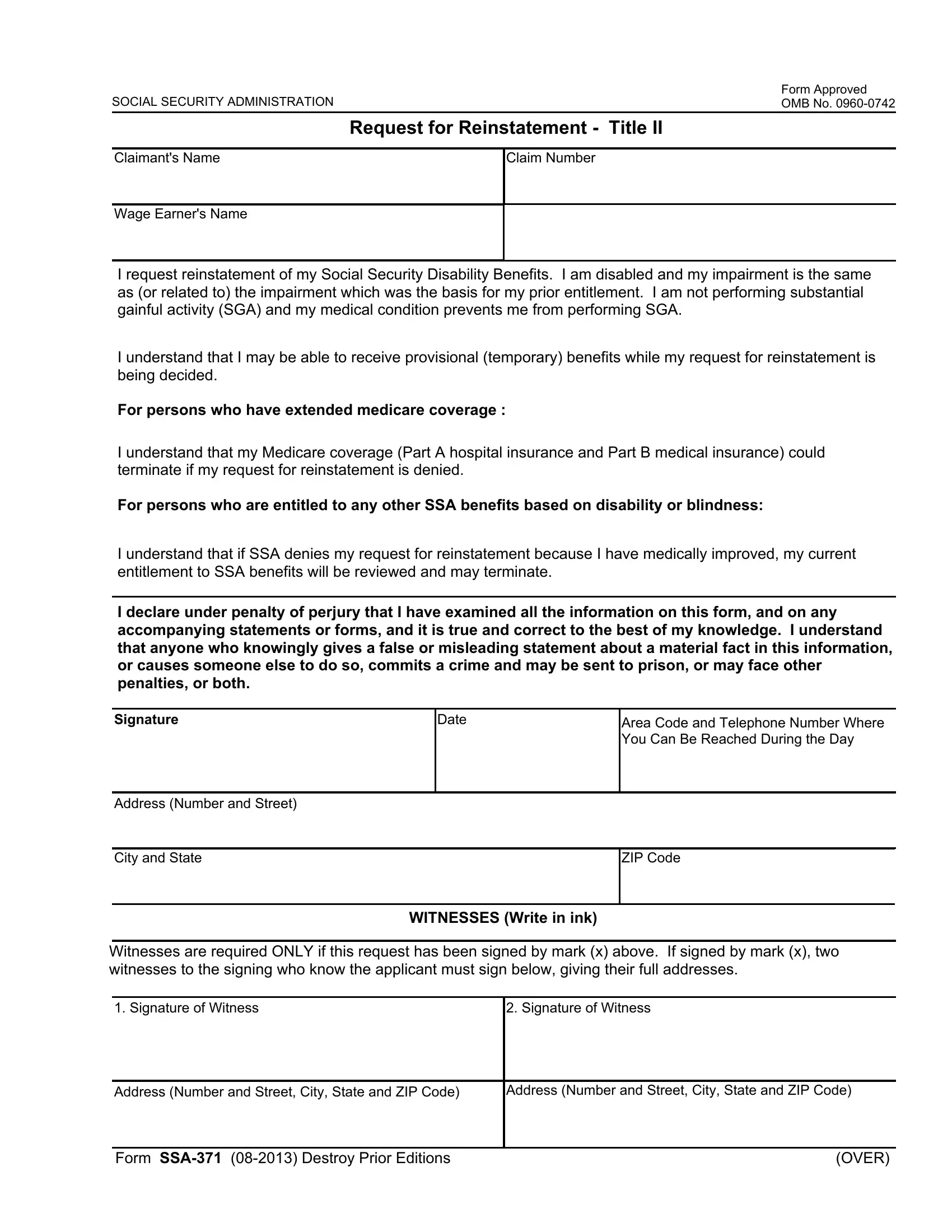
Navigating the complexities of Social Security disability benefits can be a daunting task, particularly when seeking reinstatement of these vital resources. The SSA 371 form emerges as a beacon of hope for individuals who, after a cessation of benefits, find themselves still unable to engage in substantial gainful activity due to a disabling condition. This Request for Reinstatement - Title II form is a critical document designed to facilitate the reinstatement process, requiring claimants to affirm that their disability is either the same as or related to the impairment that was the basis for their original entitlement to benefits. Moreover, it underscores the possibility of receiving provisional benefits while the reinstatement request is evaluated, adding a layer of interim support. The intricacies of this form extend to those with extended Medicare coverage, accentuating the potential implications for medical insurance should the request be denied. Importantly, the declaration under penalty of perjury reinforces the need for honesty and accuracy in the submission process, considering the severe ramifications of misleading statements. Alongside, the form includes provisions for those who might sign by mark, necessitating witness verification to uphold the integrity of the request. This process, governed by the Social Security Administration, underscores the tailored mechanisms in place to assist individuals in navigating their journey back to benefit entitlement, framing the SSA 371 form as not just a document, but as a lifeline for those in need.
| Question | Answer |
|---|---|
| Form Name | Form Ssa 371 |
| Form Length | 2 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 30 sec |
| Other names | ssa form ssa 371 for, ssa 371, ssa ssa 371 for, ssa ssa 371 |