
You can fill in CSHCN instantly with our online tool for PDF editing. FormsPal is devoted to giving you the ideal experience with our editor by constantly releasing new capabilities and improvements. Our editor has become a lot more intuitive thanks to the newest updates! So now, editing PDF forms is simpler and faster than ever. In case you are looking to get started, this is what it will require:
Step 1: Just hit the "Get Form Button" in the top section of this page to open our form editing tool. Here you will find everything that is required to work with your document.
Step 2: This tool lets you change your PDF file in many different ways. Improve it with customized text, correct what is already in the document, and add a signature - all when you need it!
It is straightforward to complete the form using this practical guide! Here's what you need to do:
1. While submitting the CSHCN, make sure to include all needed fields in the associated section. This will help facilitate the work, enabling your information to be processed efficiently and accurately.
2. Just after the last part is done, go on to enter the applicable details in all these: Client Information, Client name, CSHCN Services Program number, Date of birth, Client Address, Does the client receive therapy, If yes please indicate in the, Diagnosis Codes, Evaluation or Re Evaluation Summary, Date of evaluation or reevaluation, Service Request Indicate procedure, Procedure Code, Modifier, From Date, and Date.
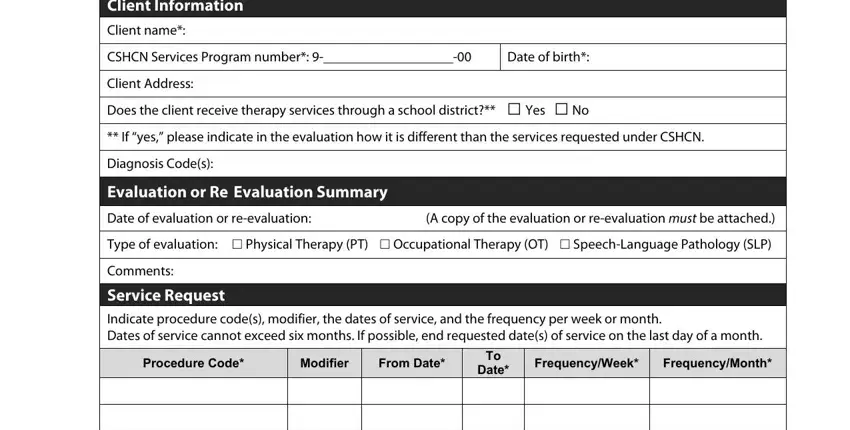
Be extremely mindful when completing Evaluation or Re Evaluation Summary and Date, since this is the section in which many people make some mistakes.
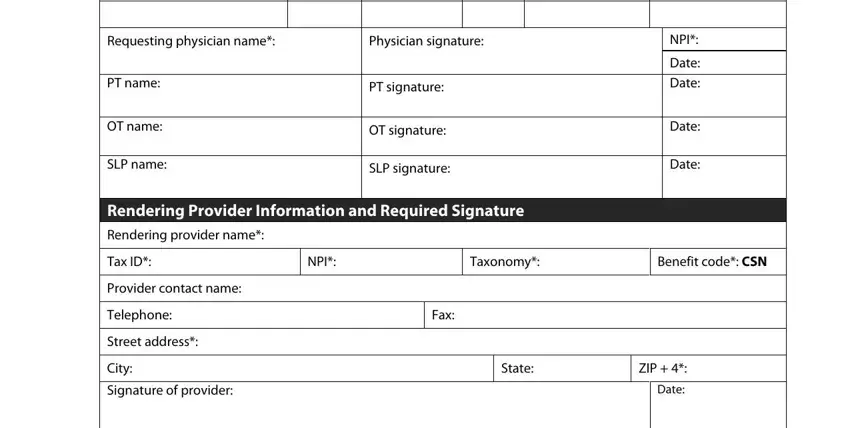
3. The following segment is about Requesting physician name, Physician signature, PT name, OT name, SLP name, PT signature, OT signature, SLP signature, NPI, Date, Date, Date, Date, Rendering Provider Information and, and Rendering provider name - fill out all these fields.
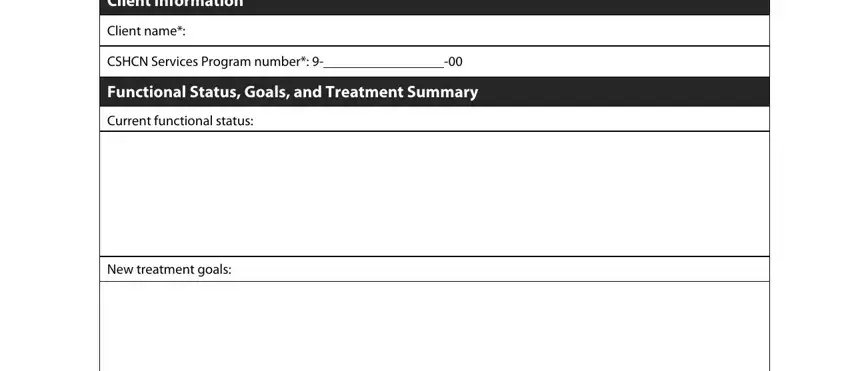
4. This specific paragraph comes next with these particular blank fields to enter your particulars in: Client Information, Client name, CSHCN Services Program number, Functional Status Goals and, Current functional status, and New treatment goals.
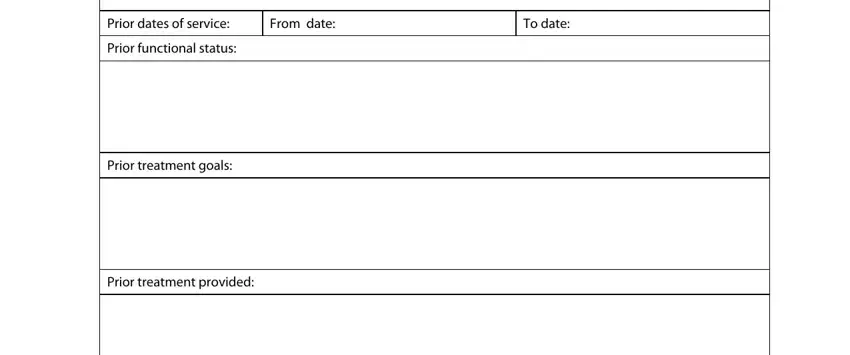
5. To finish your form, this particular segment has a number of extra blank fields. Entering Prior dates of service, From date, To date, Prior functional status, Prior treatment goals, and Prior treatment provided will wrap up everything and you'll surely be done in a tick!
Step 3: Ensure the information is right and just click "Done" to finish the task. Join us now and easily use CSHCN, all set for downloading. Every single edit made is handily saved , enabling you to modify the pdf at a later time if required. When you use FormsPal, you can certainly complete documents without the need to be concerned about personal information breaches or data entries getting shared. Our secure platform ensures that your private details are maintained safely.