
Should you need to fill out uben 100 printable, you don't have to download any sort of software - just make use of our online tool. To keep our tool on the leading edge of convenience, we aim to integrate user-driven features and improvements on a regular basis. We're always looking for suggestions - play a vital role in revampimg the way you work with PDF docs. It just takes several basic steps:
Step 1: First, access the pdf editor by pressing the "Get Form Button" in the top section of this page.
Step 2: The editor lets you change nearly all PDF files in a variety of ways. Change it by including any text, adjust existing content, and put in a signature - all doable within minutes!
Be attentive while filling in this document. Ensure that every single field is completed correctly.
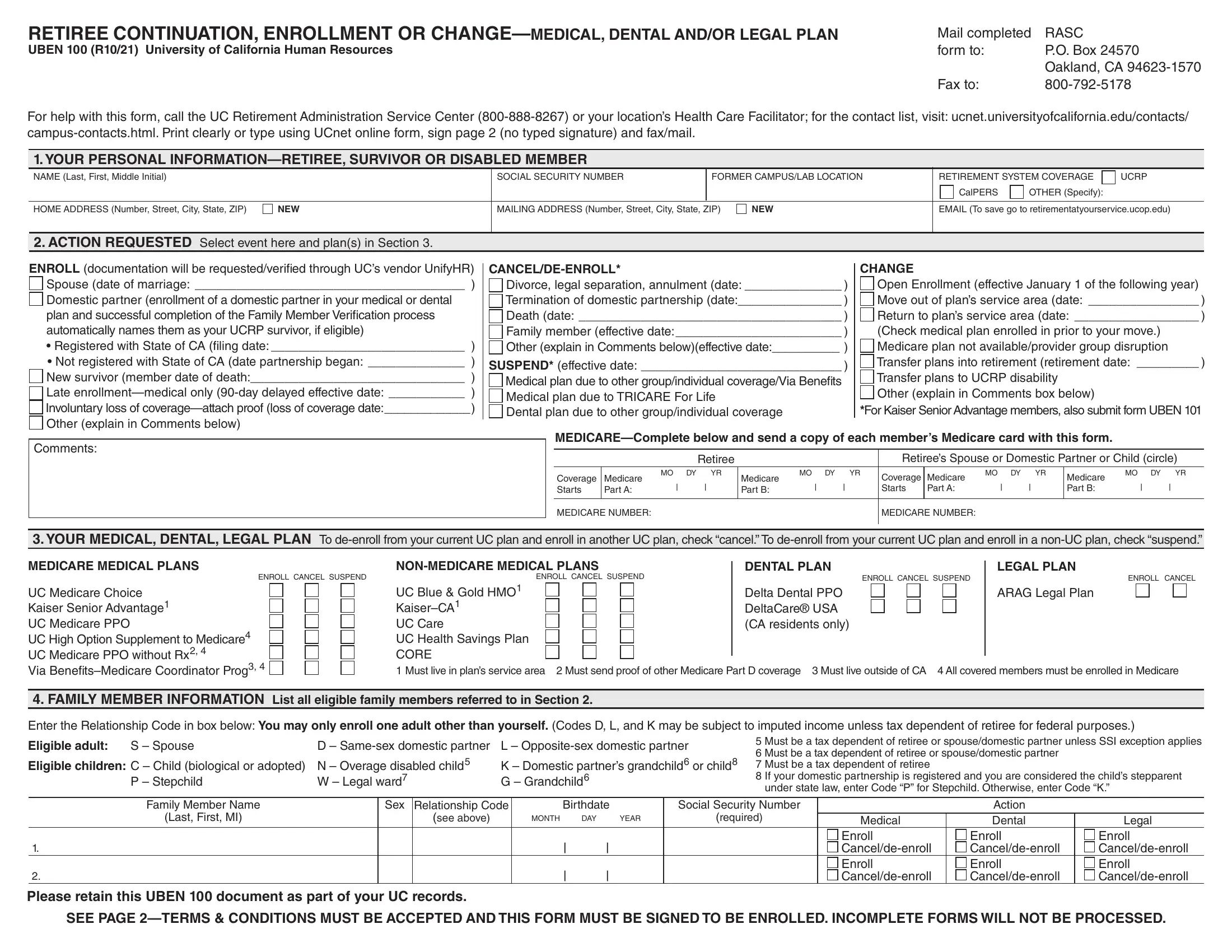
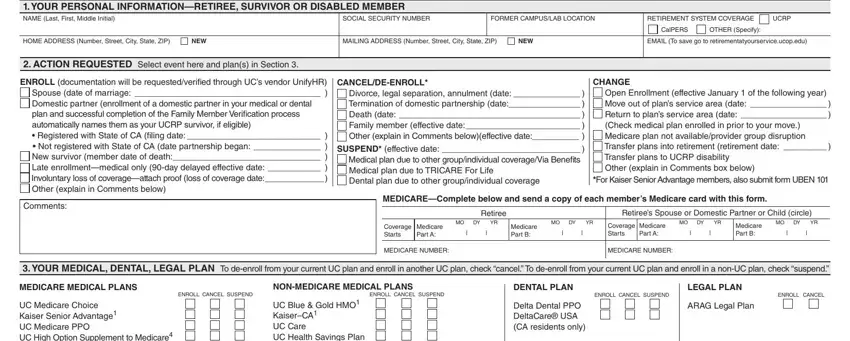
1. First, while completing the uben 100 printable, start in the form section that features the subsequent blank fields:
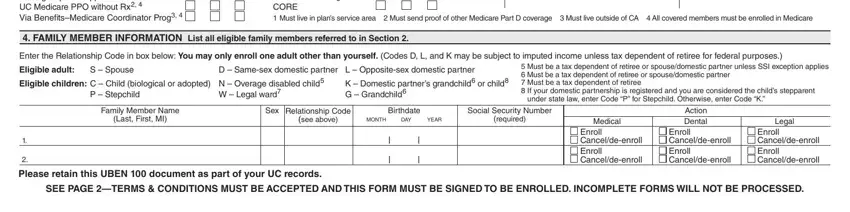
2. The next part would be to fill out these blanks: UC Medicare Choice Kaiser Senior, UC Blue Gold HMO KaiserCA UC Care, FAMILY MEMBER INFORMATION List, Enter the Relationship Code in box, S Spouse, Eligible adult Eligible children C, W Legal ward, P Stepchild, K Domestic partners grandchild or, D Samesex domestic partner L, Must be a tax dependent of, under state law enter Code P for, Family Member Name, Last First MI, and Sex Relationship Code.
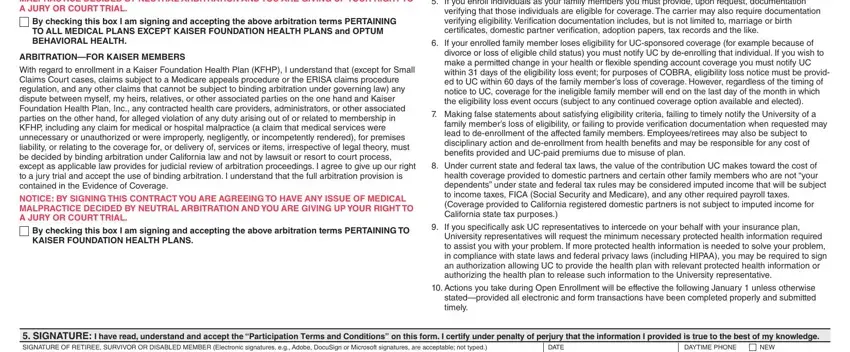
3. Completing NOTICE BY SIGNING THIS CONTRACT, By checking this box I am signing, ARBITRATIONFOR KAISER MEMBERS, With regard to enrollment in a, NOTICE BY SIGNING THIS CONTRACT, By checking this box I am signing, If you enroll individuals as your, verifying that those individuals, If your enrolled family member, divorce or loss of eligible child, Making false statements about, family members loss of eligibility, Under current state and federal, If you specifically ask UC, and University representatives will is essential for the next step, make sure to fill them out in their entirety. Don't miss any details!
4. Completing Please retain this UBEN document, and WHITE RASC YELLOW RETIREE COPY is essential in the next part - make certain that you don't rush and take a close look at each blank area!

It is easy to make a mistake while filling in your Please retain this UBEN document, and so you'll want to reread it prior to when you submit it.
Step 3: Prior to moving forward, you should make sure that blank fields were filled in the correct way. Once you believe it is all good, click “Done." Download your uben 100 printable as soon as you sign up for a free trial. Quickly gain access to the pdf file within your personal account page, together with any edits and adjustments being conveniently preserved! FormsPal is invested in the privacy of our users; we make sure that all personal information coming through our tool continues to be protected.