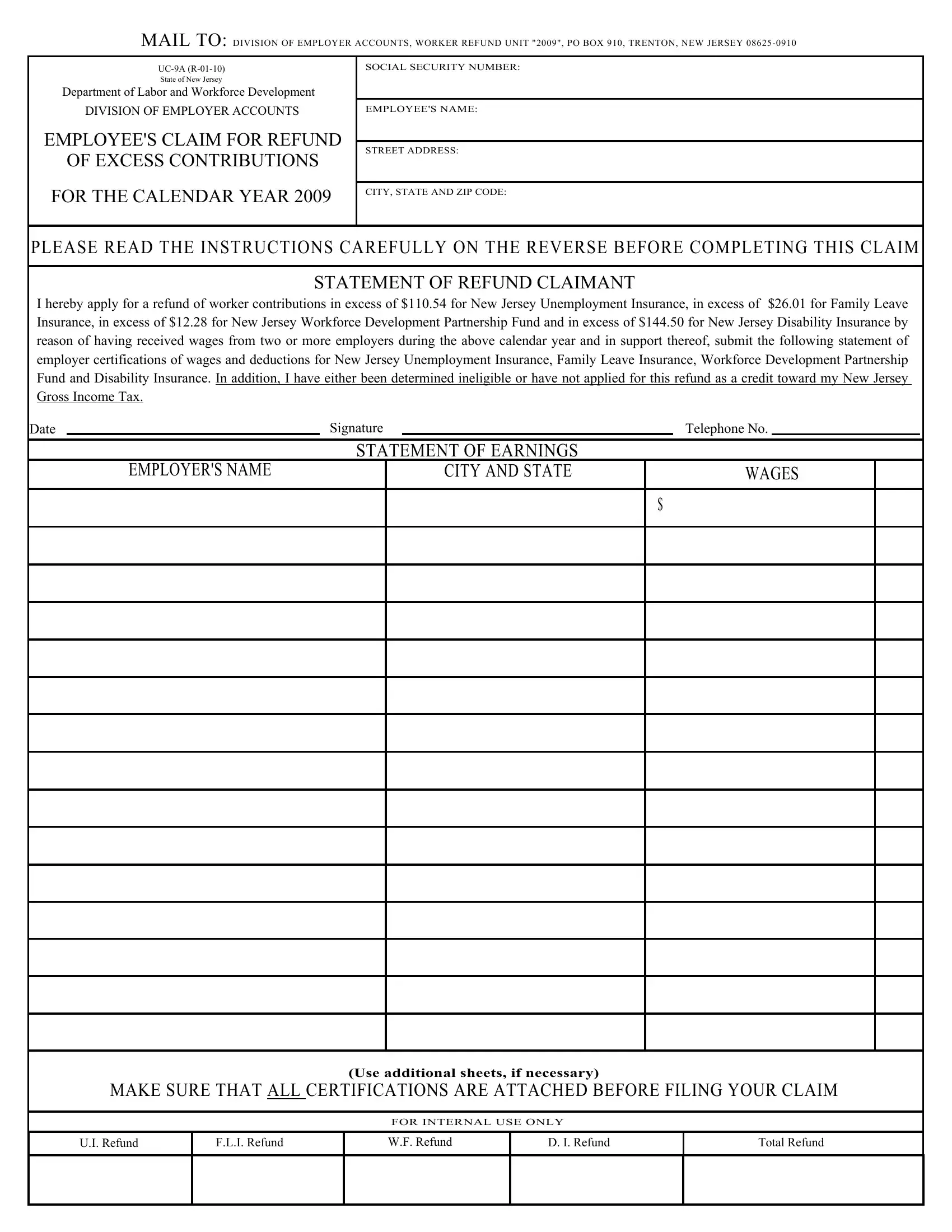
Every year, people who work in New Jersey might find themselves paying more into state-run programs than necessary. This is where the UC-9A form comes into play. Drafted by the State of New Jersey Department of Labor and Workforce Development's Division of Employer Accounts, this form serves as a request for a refund of excess contributions an employee has made towards New Jersey Unemployment Insurance, Family Leave Insurance, the Workforce Development Partnership Fund, and Disability Insurance. Specifically designed for individuals who have received wages from two or more employers during a calendar year, it addresses the scenario where deductions for these programs cumulatively exceed set maximum amounts. The form requires the claimant to meticulously list their earnings and the corresponding deductions from each employer, alongside a signed statement applying for the refund. Critical to its processing are the employer certifications of wages and deductions for the mentioned insurances, which can be obtained using a separate form or a W-2 Tax Statement. With careful consideration to detail and proper adherence to instructions—including mailing the completed form and all necessary certifications to the Division of Employer Accounts, Worker Refund Unit—applicants navigate a process that, while rigorous, offers a financial reprieve by the way of a refund. It's important to note the timeline for refunds, as no issuance occurs before August 30 of the following year, with an expected processing time of 6-8 weeks, aiming to minimize the risk of duplicate credits or refunds.
| Question | Answer |
|---|---|
| Form Name | Form Uc 9A |
| Form Length | 2 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 30 sec |
| Other names | 2009, DEDUCTED, UC-52, certifications |
MAIL TO: DIVISION OF EMPLOYER ACCOUNTS, WORKER REFUND UNIT "2009", PO BOX 910, TRENTON, NEW JERSEY
SOCIAL SECURITY NUMBER: |
|
State of New Jersey |
|
Department of Labor and Workforce Development |
|
DIVISION OF EMPLOYER ACCOUNTS |
EMPLOYEE'S NAME: |
EMPLOYEE'S CLAIM FOR REFUND |
|
|
STREET ADDRESS: |
||
OF EXCESS CONTRIBUTIONS |
||
|
||
|
|
|
FOR THE CALENDAR YEAR 2009 |
CITY, STATE AND ZIP CODE: |
|
|
PLEASE READ THE INSTRUCTIONS CAREFULLY ON THE REVERSE BEFORE COMPLETING THIS CLAIM
STATEMENT OF REFUND CLAIMANT
I hereby apply for a refund of worker contributions in excess of $110.54 for New Jersey Unemployment Insurance, in excess of $26.01 for Family Leave Insurance, in excess of $12.28 for New Jersey Workforce Development Partnership Fund and in excess of $144.50 for New Jersey Disability Insurance by reason of having received wages from two or more employers during the above calendar year and in support thereof, submit the following statement of employer certifications of wages and deductions for New Jersey Unemployment Insurance, Family Leave Insurance, Workforce Development Partnership Fund and Disability Insurance. In addition, I have either been determined ineligible or have not applied for this refund as a credit toward my New Jersey Gross Income Tax.
Date |
|
|
|
Signature |
|
|
Telephone No. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
STATEMENT OF EARNINGS |
|
|
|
|
|
||
|
|
EMPLOYER'S NAME |
|
|
CITY AND STATE |
|
WAGES |
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
$ |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
(Use additional sheets, if necessary)
MAKE SURE THAT ALL CERTIFICATIONS ARE ATTACHED BEFORE FILING YOUR CLAIM
FOR INTERNAL USE ONLY
U.I. Refund
F.L.I. Refund
W.F. Refund
D. I. Refund
Total Refund
INSTRUCTIONS FOR COMPLETING
CERTIFICATIONS
COMPLETING
1.TYPE or PRINT* your Social Security Number and your exact name and address at the top of the claim.
2.SIGN and DATE the refund claim.
3.TYPE or PRINT the exact name and location of all your employers who made deductions for New Jersey Family Leave Insurance, Workforce Development Partnership Fund, Unemployment and Disability Insurance from your 2009 wages and state the total amount of wages from which the deductions were made.
*LEGIBLE INFORMATION WILL ENSURE PROPER REIMBURSEMENT
OBTAINING CERTIFICATIONS
Your refund claim must also be accompanied by a certification of the deductions made by each of your employers listed on your claim.
Certification of your wages and deductions can be obtained through one of the following:
1.Have your employer complete form
OR
2.Furnish a copy of your
Mail the completed original
After your claim has been received it will be audited and verified. However, no refunds will be issued prior to August 30, 2010 as claims must be cross matched with Gross Income Tax records to avoid the possibility of issuing duplicate credits and/or refunds. Please allow
If you have any questions concerning your claim you may write to the above address or call
NOTE: IF THE AMOUNT DEDUCTED BY ANY ONE EMPLOYER EXCEEDS THE MAXIMUM FOR EITHER NEW JERSEY FAMILY LEAVE INSURANCE, WORKFORCE DEVELOPMENT PARTNERSHIP FUND, UNEMPLOYMENT OR DISABILITY INSURANCE, YOU SHOULD CONTACT THAT EMPLOYER FOR A REFUND OF THE BALANCE OF THE DEDUCTION.