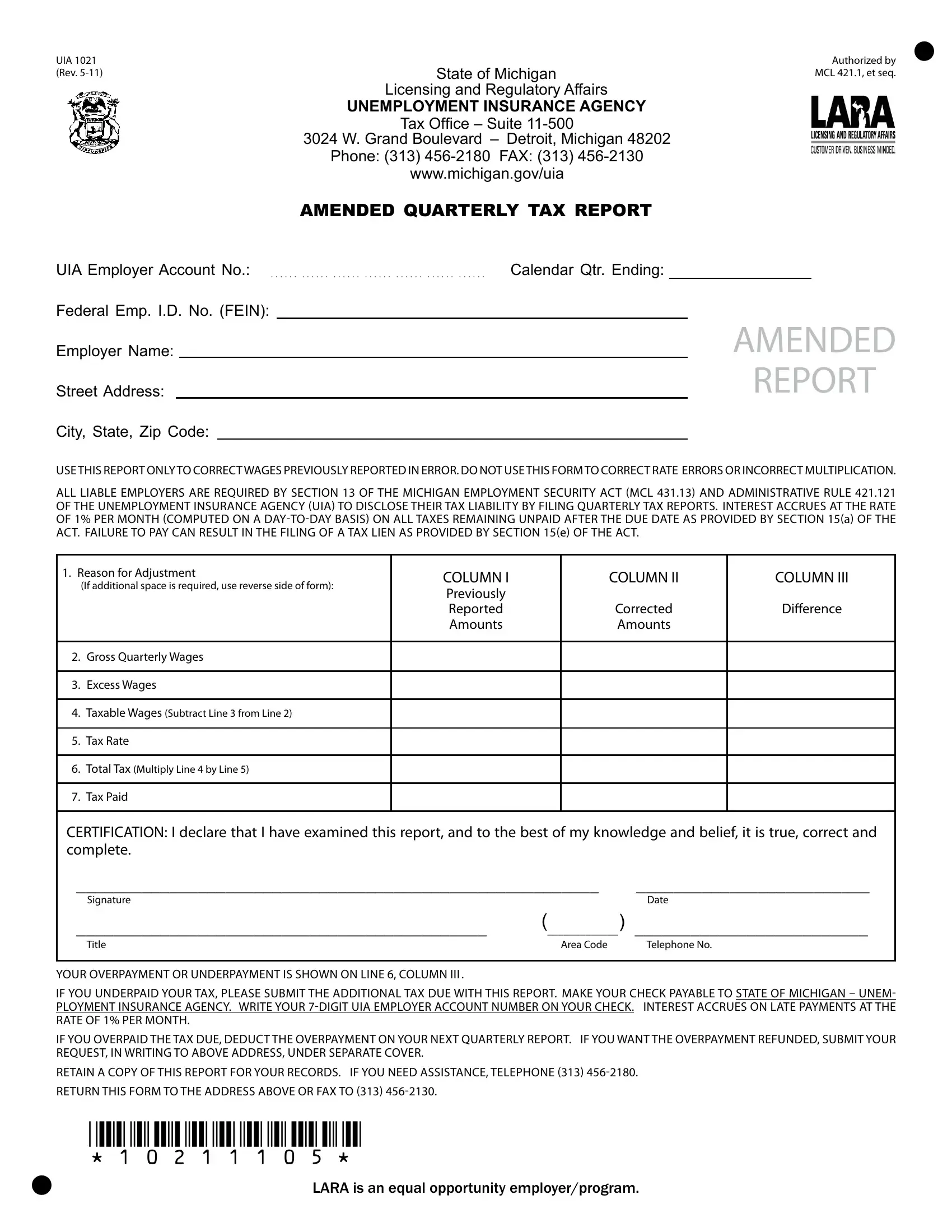
Navigating the complexities of unemployment insurance in Michigan, employers occasionally need to amend previously reported wages due to inaccuracies. This is where the UIA 1021 form, a crucial document issued by the State of Michigan Licensing and Regulatory Affairs and the Unemployment Insurance Agency, comes into play. Aimed exclusively at correcting wage reports submitted in error, the UIA 1021 form helps maintain accurate employment tax records, ensuring that both businesses and their employees are fairly represented in the state's unemployment insurance system. Its structured format requires detailed information about the employer, including the UIA Employer Account Number, Federal Employee Identification Number (FEIN), and specifics about the adjustment needed, including original and corrected figures. It's important to note that this form shouldn't be used for correcting rate errors or incorrect calculations; rather, it serves to align wage data with actual figures. The necessity of such corrections underscores the importance of precision in payroll reporting and the potential financial implications for businesses, including interest on late payments and the possibility of a tax lien if obligations remain unfulfilled. Completing and submitting the UIA 1021 accurately can prevent these outcomes, highlighting the document's significance in the broader context of employment tax compliance in Michigan.
| Question | Answer |
|---|---|
| Form Name | Form Uia 1021 |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | uia_UC1021_7608 4_7 uia 1021 form |
