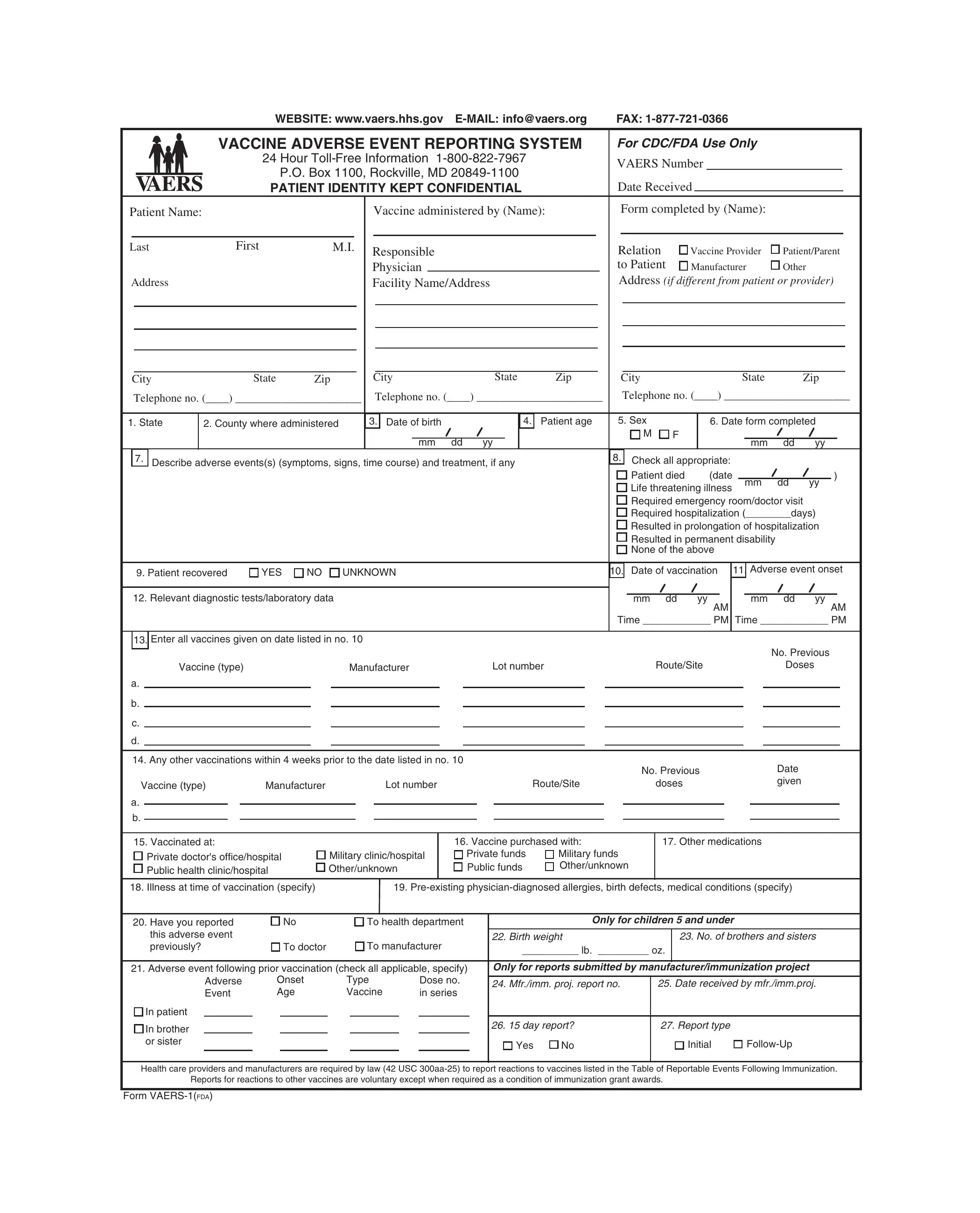
In a world where vaccine safety remains a paramount concern, the Vaccine Adverse Event Reporting System (VAERS) offers a crucial platform for gathering data on the side effects that may occur after vaccination. The VAERS-1 form is a vital component of this system, designed to be completed by vaccine providers, patients, or their guardians to report any adverse events following immunization. This form, easily accessible online and through other means such as fax or mail, ensures the confidentiality of the patient's identity while enabling a thorough documentation of the event. It captures detailed information, including patient demographics, the vaccine administered, a description of the adverse event, and any subsequent treatment received. Reporting through this system, which is mandatory for certain reactions to vaccines listed in the Reportable Events Table and encouraged for all other significant events perceived to be vaccine-related, plays a key role in identifying potential patterns that may warrant further investigation or action. Health care providers are also encouraged to notify vaccine administrators of adverse events to fulfill legal reporting obligations, ensuring a collaborative effort in monitoring vaccine safety. By contributing to a better understanding of the nature and frequency of adverse reactions, the VAERS-1 form underscores the ongoing commitment to public health and vaccine safety.
| Question | Answer |
|---|---|
| Form Name | Form Vaers 1 |
| Form Length | 2 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 30 sec |
| Other names | vaers printable form, vaers pdf, vaers online form, vaers report pdf |
WEBSITE: www.vaers.hhs.gov
|
VACCINE ADVERSE EVENT REPORTING SYSTEM |
For CDC/FDA Use Only |
|
|||
|
|
24 Hour |
VAERS Number |
|
||
|
|
P.O. Box 1100, Rockville, MD |
|
|||
|
|
|
|
|
||
|
|
PATIENT IDENTITY KEPT CONFIDENTIAL |
Date Received |
|
||
Patient Name: |
|
|
Vaccine administered by (Name): |
Form completed by (Name): |
|
|
Last |
First |
M.I. |
Responsible |
Relation |
Vaccine Provider |
Patient/Parent |
|
|
|
||||
|
|
|
Physician |
to Patient |
Manufacturer |
Other |
Address |
|
|
Facility Name/Address |
Address (if different from patient or provider) |
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
City |
|
|
|
State |
|
Zip |
|
|
City |
State |
Zip |
City |
|
|
|
|
|
State |
|
Zip |
|
|
|
|
||||||||||||||||
|
Telephone no. (____) ______________________ Telephone no. (____) ______________________ |
Telephone no. (____) ______________________ |
|||||||||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
1. State |
|
2. County where administered |
|
|
3. |
Date of birth |
|
4. |
Patient age |
5. Sex |
|
|
6. Date form completed |
|
|
|
|
||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
M |
F |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
mm dd |
yy |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
mm |
dd |
yy |
|
|
|
|
|||
|
7. |
|
|
Describe adverse events(s) (symptoms, signs, time course) and treatment, if any |
|
|
|
|
8. |
Check all appropriate: |
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||
|
|
|
|
|
|
|
|
|
Patient died |
|
(date |
|
|
|
|
|
|
) |
|
|
|
||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Life threatening illness |
|
mm |
dd |
yy |
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Required emergency room/doctor visit |
|
|
|
|
|
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Required hospitalization (________days) |
|
|
|
|
|||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Resulted in prolongation of hospitalization |
|
|
|
|
|||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Resulted in permanent disability |
|
|
|
|
|
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
None of the above |
|
|
|
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||
|
9. Patient recovered |
YES |
NO |
UNKNOWN |
|
|
|
|
|
|
|
10. |
Date of vaccination |
11. |
Adverse event onset |
||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
12. Relevant diagnostic tests/laboratory data |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
mm |
dd |
yy |
AM |
|
|
|
mm |
dd |
yy |
AM |
|||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Time ____________ PM |
Time ____________ PM |
|||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||
|
13. |
Enter all vaccines given on date listed in no. 10 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
No. Previous |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
Vaccine (type) |
|
|
|
|
Manufacturer |
Lot number |
|
|
Route/Site |
|
|
|
|
|
|
|
Doses |
|
|
|
|
|||||||||||||||
|
a. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
b. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
c. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
d. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||
|
14. Any other vaccinations within 4 weeks prior to the date listed in no. 10 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Date |
|
|
|
|
|
||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
No. Previous |
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
Vaccine (type) |
Manufacturer |
|
|
|
Lot number |
|
|
|
Route/Site |
|
|
doses |
|
|
|
|
|
|
|
|
given |
|
|
|
|
|
||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||
a.
b.
15. Vaccinated at: |
|
Private doctor's office/hospital |
Military clinic/hospital |
Public health clinic/hospital |
Other/unknown |
16. Vaccine purchased with:
Private funds |
Military funds |
Public funds |
Other/unknown |
17. Other medications
18. Illness at time of vaccination (specify) |
|
|
19. |
||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
20. Have you reported |
|
No |
|
To health department |
|
|
Only for children 5 and under |
|
|||||||
this adverse event |
|
|
|
To manufacturer |
22. Birth weight |
|
|
23. No. of brothers and sisters |
|||||||
previously? |
|
To doctor |
|
__________ lb. _________ oz. |
|
|
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
||||||
21. Adverse event following prior vaccination (check all applicable, specify) |
Only for reports submitted by manufacturer/immunization project |
||||||||||||||
|
Adverse |
Onset |
Type |
|
|
Dose no. |
|
|
|
|
|
|
|||
|
|
|
24. Mfr./imm. proj. report no. |
25. Date received by mfr./imm.proj. |
|||||||||||
|
Event |
Age |
Vaccine |
|
|
in series |
|||||||||
|
|
|
|
|
|
|
|
|
|||||||
In patient |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
In brother |
|
|
|
|
|
|
|
|
|
26. 15 day report? |
|
27. Report type |
|
||
or sister |
|
|
|
|
|
|
|
|
Yes |
No |
|
|
Initial |
||
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Health care providers and manufacturers are required by law (42 USC
Form
"Fold in thirds, tape & mail — DO NOT STAPLE FORM"
NO POSTAGE
NECESSARY
IF MAILED
IN THE
UNITED STATES
OR APO/FPO
BUSINESS REPLY MAIL
POSTAGE WILL BE PAID BY ADDRESSEE
VAERS
P.O. Box 1100
Rockville MD
DIRECTIONS FOR COMPLETING FORM
(Additional pages may be attached if more space is needed.)
GENERAL
•Use a separate form for each patient. Complete the form to the best of your abilities. Items 3, 4, 7, 8, 10, 11, and 13 are considered essential and should be completed whenever possible. Parents/Guardians may need to consult the facility where the vaccine was administered for some of the information (such as manufacturer, lot number or laboratory data.)
•Refer to the Reportable Events Table (RET) for events mandated for reporting by law. Reporting for other serious events felt to be related but not on the RET is encouraged.
•Health care providers other than the vaccine administrator (VA) treating a patient for a suspected adverse event should notify the VA and provide the information about the adverse event to allow the VA to complete the form to meet the VA's legal responsibility.
•These data will be used to increase understanding of adverse events following vaccination and will become part of CDC Privacy Act System
•Postage will be paid by addressee. Forms may be photocopied (must be front & back on same sheet).
SPECIFIC INSTRUCTIONS
Form Completed By: To be used by parents/guardians, vaccine manufacturers/distributors, vaccine administrators, and/or the person completing the form on behalf of the patient or the health professional who administered the vaccine.
Item 7: Describe the suspected adverse event. Such things as temperature, local and general signs and symptoms, time course, duration of symptoms, diagnosis, treatment and recovery should be noted.
Item 9: Check "YES" if the patient's health condition is the same as it was prior to the vaccine, "NO" if the patient has not returned to the
Item 10: Give dates and times as specifically as you can remember. If you do not know the exact time, please
and 11: indicate "AM" or "PM" when possible if this information is known. If more than one adverse event, give the onset date and time for the most serious event.
Item 12: Include "negative" or "normal" results of any relevant tests performed as well as abnormal findings.
Item 13: List ONLY those vaccines given on the day listed in Item 10.
Item 14: List any other vaccines that the patient received within 4 weeks prior to the date listed in Item 10.
Item 16: This section refers to how the person who gave the vaccine purchased it, not to the patient's insurance.
Item 17: List any prescription or
Item 18: List any short term illnesses the patient had on the date the vaccine(s) was given (i.e., cold, flu, ear infection).
Item 19: List any
Item 21: List any suspected adverse events the patient, or the patient's brothers or sisters, may have had to previous vaccinations. If more than one brother or sister, or if the patient has reacted to more than one prior vaccine, use additional pages to explain completely. For the onset age of a patient, provide the age in months if less than two years old.
Item 26: This space is for manufacturers' use only.