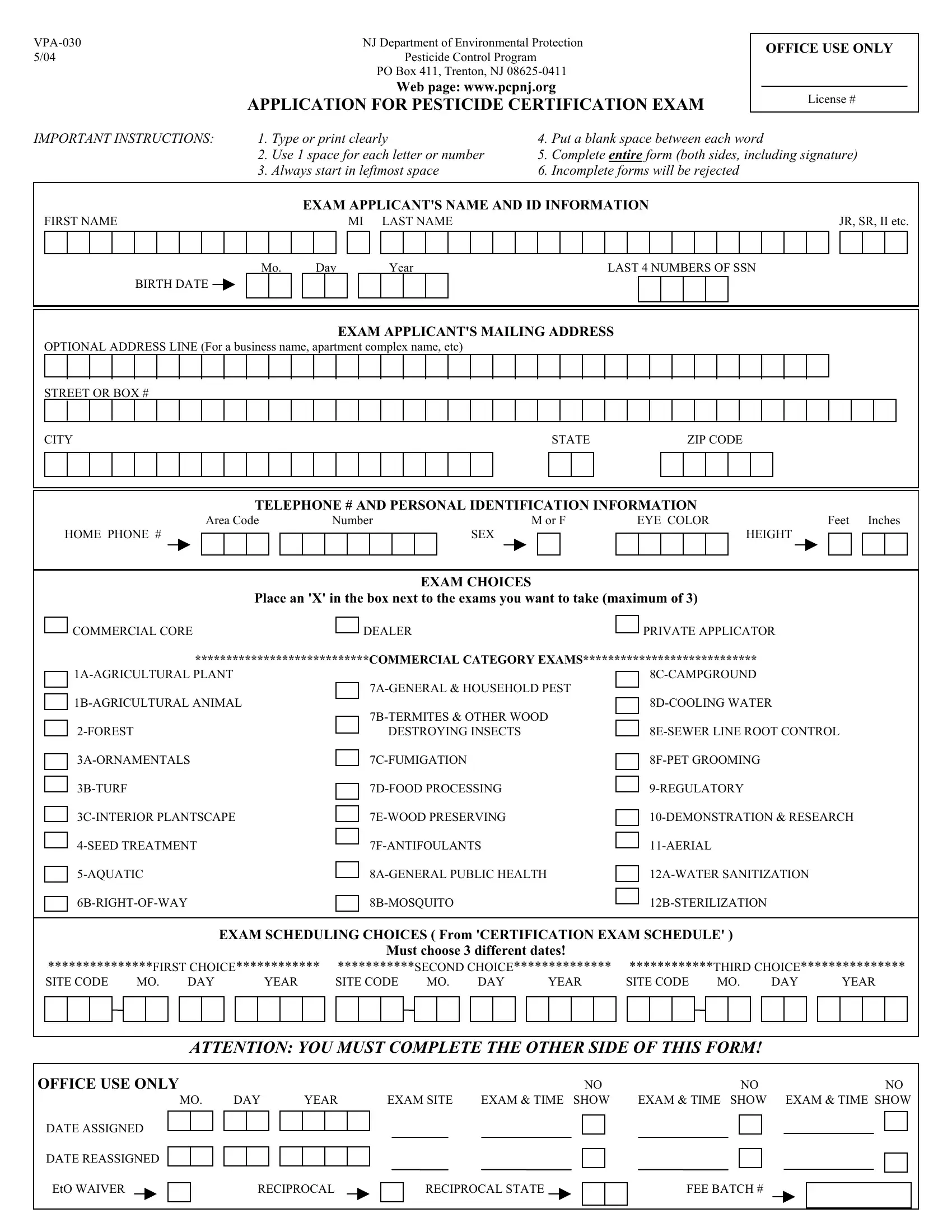
Navigating the path to becoming a certified pesticide applicator in New Jersey entails navigating through a sea of paperwork and guidelines. At the forefront of this journey is the VPA-030 form, a critical document issued by the NJ Department of Environmental Protection's Pesticide Control Program. This form serves as an application for the pesticide certification exam, a pivotal step for those seeking to earn or renew their credentials in the field. With its comprehensive nature, the form demands attention to detail, from the personal identification information to specifying the categories of examinations the applicant wishes to undertake. Whether you aim for a commercial core, dealer, private applicator, or a specific commercial category exam, understanding the nuances of the VPA-030 form is paramount. Completing it accurately and in its entirety, including the applicant's signature and adherence to the listed instructions, is the first step toward achieving certification. Moreover, this process underscores the significance of honesty and accuracy, as any misleading information could result in the denial or revocation of certification. For those navigating this path, the form also includes sections for employment details and a check for training verification, reflecting the state's commitment to ensuring qualified, knowledgeable individuals serve in this critical industry.
| Question | Answer |
|---|---|
| Form Name | Form Vpa 030 |
| Form Length | 4 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 1 min |
| Other names | 7D-FOOD, 3C-INTERIOR, New_Jersey, www guruscamp com |
NJ Department of Environmental Protection |
|
5/04 |
Pesticide Control Program |
PO Box 411, Trenton, NJ
Web page: www.pcpnj.org
APPLICATION FOR PESTICIDE CERTIFICATION EXAM
OFFICE USE ONLY
License #
IMPORTANT INSTRUCTIONS: |
1. Type or print clearly |
4. |
Put a blank space between each word |
||||||||||||||||||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
2. |
Use 1 space for each letter or number |
5. |
Complete ENTIRE form (both sides, including signature) |
|||||||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
3. |
Always start in leftmost space |
6. |
Incomplete forms will be rejected |
|||||||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
EXAM APPLICANT'S NAME AND ID INFORMATION |
|||||||||||||||||||||||||||||||||||||
FIRST NAME |
|
|
|
|
|
|
|
MI |
LAST NAME |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
JR, SR, II etc. |
|||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Mo. |
|
|
Day |
Year |
|
|
|
|
|
LAST 4 NUMBERS OF SSN |
||||||||||||||||||||||||||||||
|
|
|
|
|
BIRTH DATE |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
EXAM APPLICANT'S MAILING ADDRESS
OPTIONAL ADDRESS LINE (For a business name, apartment complex name, etc)
STREET OR BOX #
CITY |
|
STATE |
|
|
ZIP CODE |
|||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
TELEPHONE # AND PERSONAL IDENTIFICATION INFORMATION
Area Code |
Number |
HOME PHONE #
M or F
SEX
EYE COLOR |
|
|
Feet Inches |
||||||||
|
|
|
|
|
HEIGHT |
|
|
|
|
||
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
EXAM CHOICES
Place an 'X' in the box next to the exams you want to take (maximum of 3)
COMMERCIAL CORE |
|
DEALER |
|
PRIVATE APPLICATOR |
|
|
|||
****************************COMMERCIAL CATEGORY EXAMS**************************** |
||||
|
|
|||
|
|
|||
|
|
|||
|
|
|||
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
DESTROYING INSECTS |
|
||
|
|
|||
|
|
|||
|
|
|||
|
|
|||
|
|
|||
|
|
|||
|
|
|||
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|||
|
|
|||
|
|
|
|
|
|
|
|||
|
|
|||
|
|
|||
|
|
|||
|
|
|||
|
|
|||
|
|
|
|
|
|
|
|
|
EXAM SCHEDULING CHOICES ( From 'CERTIFICATION EXAM SCHEDULE' ) |
|
|
|
|
|
|
|
||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Must choose 3 different dates! |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||
***************FIRST CHOICE************ |
|
***********SECOND CHOICE************** |
|
************THIRD CHOICE*************** |
||||||||||||||||||||||||||||||||||||||||
SITE CODE |
|
MO. |
|
DAY |
|
|
|
YEAR |
SITE CODE |
|
MO. |
DAY |
|
|
YEAR |
SITE CODE |
|
MO. |
DAY |
|
|
YEAR |
||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
ATTENTION: YOU MUST COMPLETE THE OTHER SIDE OF THIS FORM!
OFFICE USE ONLY |
|
|
|
|
|
|
|
|
|
|
|
|
|
NO |
|
|
NO |
|
|
NO |
|||||
|
MO. |
|
DAY |
|
|
YEAR |
EXAM SITE EXAM & TIME SHOW |
EXAM & TIME SHOW |
EXAM & TIME SHOW |
||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
DATE ASSIGNED |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
DATE REASSIGNED |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
EtO WAIVER
RECIPROCAL
RECIPROCAL STATE
FEE BATCH #
EMPLOYER NAME AND TELEPHONE NUMBER
IF YOUR EMPLOYER IS A LICENSED PESTICIDE APPLICATOR BUSINESS OR PESTICIDE DEALER BUSINESS, PLEASE FILL IN THE
BUSINESS LICENSE NUMBER HERE
IN ALL CASES, PROVIDE ALL OF THE FOLLOWING INFORMATION
EMPLOYER NAME OR BUSINESS NAME (pesticide
Area Code |
Number |
EMPLOYER OR BUSINESS TELEPHONE #
IF NO CURRENT EMPLOYER OR BUSINESS, FILL IN HOME PHONE #
|
EMPLOYER OR BUSINESS MAIL ADDRESS |
|
|
|
|
IF NO CURRENT EMPLOYER OR BUSINESS, FILL IN HOME MAIL ADDRESS |
|
|
|
STREET OR BOX # |
|
|
|
|
CITY |
STATE |
ZIP CODE |
COUNTY |
USE |
|
|
|
|
COUNTY |
|
|
|
|
CODE |
|
|
|
|
BELOW |
EMPLOYER OR BUSINESS PHYSICAL ADDRESS
IF NO CURRENT EMPLOYER OR BUSINESS, FILL IN HOME PHYSICAL ADDRESS
STREET
CITY |
STATE |
ZIP CODE |
COUNTY |
USE
COUNTY
CODE
BELOW
SIGNATURE BOX
SIGNATURE OF EXAM APPLICANT
EXAM APPLICATION FORM WILL BE REJECTED WITHOUT THIS SIGNATURE!!
NOTE: Providing false or misleading information on this form will result in denial or revocation of your certification and licensing.
|
|
|
COUNTY CODES |
|
|
01 |
- Atlantic County |
08 |
- Gloucester County |
15 |
- Ocean County |
02 |
- Bergen County |
09 |
- Hudson County |
16 |
- Passaic County |
03 |
- Burlington County |
10 |
- Hunterdon County |
17 |
- Salem County |
04 |
- Camden County |
11 |
- Mercer County |
18 |
- Somerset County |
05 |
- Cape May County |
12 |
- Middlesex County |
19 |
- Sussex County |
06 |
- Cumberland County |
13 |
- Monmouth County |
20 |
- Union County |
07 |
- Essex County |
14 |
- Morris County |
21 |
- Warren County |
|
|
|
|
22 |
– Out of State |
|
|
|
|
|
|
State of New Jersey
Richard J.Codey |
Department of Environmental Protection |
Bradley M. Campbell |
Acting Governor |
|
Commissioner |
|
Pesticide Control Program |
|
|
PO Box 411 |
|
|
Trenton, NJ |
|
COMMERCIAL PESTICIDE APPLICATOR
CATEGORY TRAINING VERIFICATION FORM
PLEASE CHECK APPROPRIATE BOX BELOW:
YES, I HAVE COMPLETED THE 40 HOURS OF “ON THE JOB TRAINING” AND HAVE PERFORMED/WITNESSED THE MINIMUM NUMBER OF PESTICIDE APPLICATIONS REQUIRED BY NJAC
___________________________________________________________________________
NO, I HAVE NOT COMPLETED THE 40 HOURS OF
Please explain below why training is not available:
APPLICANT’S NAME (print):______________________________________________________
APPLICANT’S SIGNATURE: _______________________________DATE: ________________
TRAINER: By signing below, I verify that the above named person completed 40 hours of
TRAINER’S NAME (print): _________________________________________________________
TRAINER’S PESTICIDE APPLICATOR LICENSE #: ____________________________________
TRAINER’S SIGNATURE: ______________________________________ DATE: _____________
Note: This form is for Commercial Pesticide Applicator licensing only. Please do not submit with Commercial Pesticide Operator application forms.
catrainingform 11/04
State of New Jersey
Richard J.Codey |
Department of Environmental Protection |
Bradley M. Campbell |
Acting GOVERNOR |
|
COMMISSIONER |
|
Pesticide Control Program |
|
|
PO Box 411 |
|
|
Trenton, NJ |
|
|
“AFFIDAVIT” |
|
I the undersigned attest that I have the required
_______________________________________________________________________
Upon this Department’s request, copies of my pesticide application records, employer’s statements and any other proof as deemed necessary by the Department will be provided.
I hereby swear/affirm that the aforementioned statement is true to the best of my knowledge:
Print name: _____________________________________________________________
Signature: ___________________________________________ Date: ______________
Please Note: Only complete this affidavit if you have at least one year of work experience in the categories you are applying for. Do not send in the “Category Training Verification Form” when using this affidavit.
affidavit 2/05