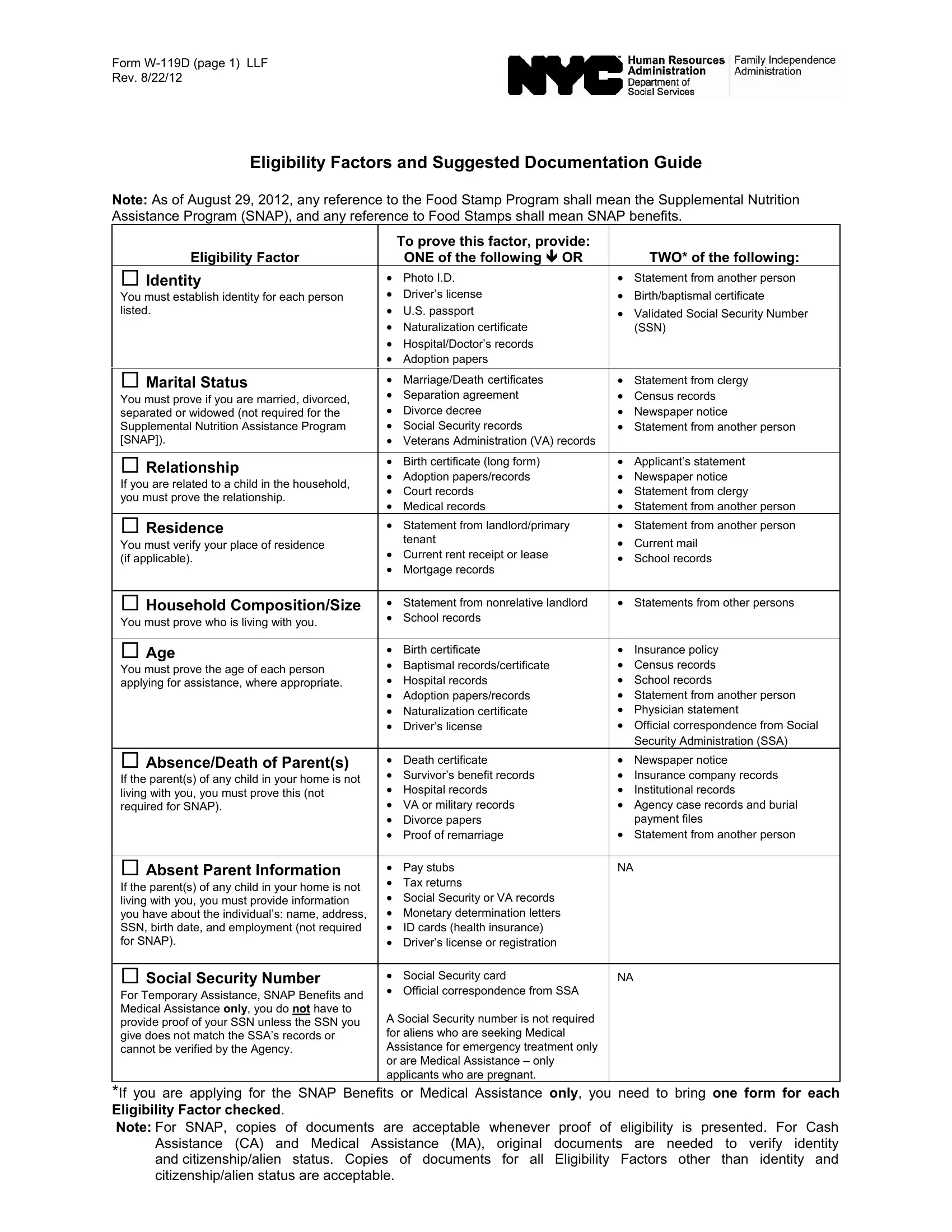
In the realm of assistance programs, the Form W-119D serves as a crucial document, guiding individuals through the eligibility verification process for various support services including the Supplemental Nutrition Assistance Program (SNAP), Cash Assistance (CA), and Medical Assistance (MA). Updated on August 22, 2012, this form reflects changes in terminology, with references to the Food Stamp Program updated to SNAP, underscoring the program's evolution. The form is extensive, detailing the necessary documentation to establish eligibility factors such as identity, marital status, relationship, residence, household composition, age, and the circumstances surrounding the absence or death of a parent. It extends into specific requirements for proving citizenship or current alien status, different income sources (both earned and unearned), resources, shelter expenses, and medical expenses, among others. Each section of the form specifies the types of documents acceptable, ranging from personal identification and official records to statements from third parties and financial records, providing a comprehensive guide for applicants to substantiate their eligibility. Importantly, the form differentiates between documentation required for SNAP, where copies are permissible, and CA and MA, which often require original documents, highlighting the tailored approach to verifying eligibility across different assistance programs. Through these meticulous documentation requirements, the Form W-119D plays a pivotal role in ensuring that assistance is provided to those genuinely eligible, thereby upholding the integrity and purpose of these vital support services.
| Question | Answer |
|---|---|
| Form Name | Form W 119D |
| Form Length | 4 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 1 min |
| Other names | Keogh, w119d, w 119d, SSI |

Form
Rev. 8/22/12
Eligibility Factors and Suggested Documentation Guide
Note: As of August 29, 2012, any reference to the Food Stamp Program shall mean the Supplemental Nutrition Assistance Program (SNAP), and any reference to Food Stamps shall mean SNAP benefits.
|
|
To prove this factor, provide: |
|
|
|
Eligibility Factor |
|
ONE of the following OR |
|
TWO* of the following: |
|
Identity |
• |
Photo I.D. |
• Statement from another person |
||
• |
|
• |
|
||
You must establish identity for each person |
Driver’s license |
Birth/baptismal certificate |
|||
listed. |
• |
U.S. passport |
• Validated Social Security Number |
||
|
• |
Naturalization certificate |
|
(SSN) |
|
|
• |
Hospital/Doctor’s records |
|
|
|
|
• |
Adoption papers |
|
|
|
|
|
|
|
|
|
Marital Status |
• |
Marriage/Death certificates |
• |
Statement from clergy |
|
• |
Separation agreement |
• |
|
||
You must prove if you are married, divorced, |
Census records |
||||
• |
|
• |
|
||
separated or widowed (not required for the |
Divorce decree |
Newspaper notice |
|||
Supplemental Nutrition Assistance Program |
• |
Social Security records |
• Statement from another person |
||
[SNAP]). |
• |
Veterans Administration (VA) records |
|
|
|
|
|
|
|
|
|
Relationship |
• |
Birth certificate (long form) |
• |
Applicant’s statement |
|
• |
Adoption papers/records |
• |
Newspaper notice |
||
If you are related to a child in the household, |
|||||
• |
Court records |
• |
Statement from clergy |
||
you must prove the relationship. |
|||||
• |
Medical records |
• Statement from another person |
|||
|
|||||
Residence |
• |
Statement from landlord/primary |
• Statement from another person |
||
|
tenant |
• |
|
||
You must verify your place of residence |
|
Current mail |
|||
• |
|
||||
(if applicable). |
Current rent receipt or lease |
• |
School records |
||
• |
|
||||
|
Mortgage records |
|
|
||
|
|
|
|
||
Household Composition/Size |
• |
Statement from nonrelative landlord |
• Statements from other persons |
||
• |
School records |
|
|
||
You must prove who is living with you. |
|
|
|||
|
|
|
|
||
|
|
|
|
|
|
Age |
• |
Birth certificate |
• |
Insurance policy |
|
• |
Baptismal records/certificate |
• |
Census records |
||
You must prove the age of each person |
|||||
• |
|
• |
School records |
||
applying for assistance, where appropriate. |
Hospital records |
||||
|
• |
Adoption papers/records |
• Statement from another person |
||
|
• |
Naturalization certificate |
• |
Physician statement |
|
|
• |
Driver’s license |
• Official correspondence from Social |
||
|
|
|
|
Security Administration (SSA) |
|
Absence/Death of Parent(s) |
• |
Death certificate |
• |
Newspaper notice |
|
• |
Survivor’s benefit records |
• |
Insurance company records |
||
If the parent(s) of any child in your home is not |
|||||
• |
Hospital records |
• |
Institutional records |
||
living with you, you must prove this (not |
|||||
required for SNAP). |
• |
VA or military records |
• Agency case records and burial |
||
|
• |
Divorce papers |
|
payment files |
|
|
• |
Proof of remarriage |
• Statement from another person |
||
|
|
|
|
|
|
Absent Parent Information |
• |
Pay stubs |
NA |
|
|
• |
Tax returns |
|
|
||
If the parent(s) of any child in your home is not |
|
|
|||
• |
Social Security or VA records |
|
|
||
living with you, you must provide information |
|
|
|||
you have about the individual’s: name, address, |
• |
Monetary determination letters |
|
|
|
SSN, birth date, and employment (not required |
• |
ID cards (health insurance) |
|
|
|
for SNAP). |
• |
Driver’s license or registration |
|
|
|
|
|
|
|
|
|
Social Security Number |
• |
Social Security card |
NA |
|
|
For Temporary Assistance, SNAP Benefits and |
• Official correspondence from SSA |
|
|
||
|
|
|
|
||
Medical Assistance only, you do not have to |
A Social Security number is not required |
|
|
||
provide proof of your SSN unless the SSN you |
|
|
|||
for aliens who are seeking Medical |
|
|
|||
give does not match the SSA’s records or |
|
|
|||
|
|
|
|
||
cannot be verified by the Agency. |
Assistance for emergency treatment only |
|
|
||
|
or are Medical Assistance – only |
|
|
||
|
applicants who are pregnant. |
|
|
||
*If you are applying for the SNAP Benefits or Medical Assistance only, you need to bring one form for each Eligibility Factor checked.
Note: For SNAP, copies of documents are acceptable whenever proof of eligibility is presented. For Cash Assistance (CA) and Medical Assistance (MA), original documents are needed to verify identity and citizenship/alien status. Copies of documents for all Eligibility Factors other than identity and citizenship/alien status are acceptable.
Form |
Human Resources Administration |
Rev. 8/22/12 |
Family Independence Administration |
Eligibility Factor |
|
To prove this factor, provide ONE of the following: |
|
Citizenship or Current Alien Status |
• |
Birth certificate |
|
• |
Baptismal certificate/records |
||
Status – U.S. citizens are eligible for Temporary Assistance, the |
|||
• |
Hospital records |
||
Supplemental Nutrition Assistance Program and medical |
|||
• |
U.S. passport |
||
assistance. Aliens must be in satisfactory immigration status in |
|||
• |
Military service records |
||
order to be eligible for Temporary Assistance, the Supplemental |
|||
Nutrition Assistance Program and medical assistance. Immigration |
• |
Naturalization certificate |
|
status is not an eligibility factor for pregnant women or immigrant |
• |
USCIS documentation |
|
children applying for Child Health Plus B. Undocumented |
• |
Evidence of continuous U.S. residence since prior to 1/1/72 |
|
immigrants and temporary nonimmigrants are eligible only for the |
|
|
|
treatment of an emergency medical condition. |
|
|
|
Earned Income |
|
|
|
|
• Current wage stubs and statements of tips |
||
|
• |
Pay envelopes |
|
From employer |
• |
Contact with employer |
|
|
• On letterhead, rate of pay per hour, hours worked per week, |
||
|
|
first pay date, if new and employer’s phone number |
|
|
• |
Business records |
|
|
• |
Tax records |
|
From |
• |
Records and related materials concerning |
|
|
|
earnings and expenses |
|
|
• Current income tax return |
||
|
• |
Current contribution check |
|
Income from rent or room/board |
• |
Statement from roomer, boarder, tenant |
|
|
• |
Income tax record |
|
Unearned Income |
|
|
|
|
• Statement from Family Court |
||
|
• Statement from person paying support |
||
Child Support |
• |
Check stubs |
|
|
• Official correspondence from the Child Support Enforcement |
||
|
|
Unit |
|
|
• |
Current award certificate |
|
Unemployment Insurance Benefits (UIB) |
• |
Official correspondence with New York State Department of |
|
|
|
Labor |
|
|
• |
Current award certificate/letter |
|
Social Security benefits (including SSI) |
• |
Current benefit check |
|
|
• Official correspondence from SSA |
||
|
• Veterans Administration official correspondence |
||
Veteran’s benefits |
• |
Current award certificate/letter |
|
|
• |
Current benefit check |
|
Worker’s Compensation |
• |
Award certificate/letter |
|
• |
Check stub |
||
|
|||
|
• |
Statement from school |
|
Education grants and loans |
• |
Statement from bank |
|
|
• Statement from agency administering grant/award letter |
||
Interest/dividends/royalties |
• Statement from bank or credit union |
||
• Statement from broker/financial institution/agent |
|||
|
|||
|
• |
Current award letter |
|
|
• |
Current benefit check |
|
Private pension/annuity |
• |
Official correspondence from source of income |
|
|
• Contact with source of income |
||
|
• |
Current contribution check |
|
Note: For SNAP, copies of documents are acceptable whenever proof of eligibility is presented. For Cash
Assistance (CA) and Medical Assistance (MA), original |
documents are needed to verify identity |
and citizenship/alien status. Copies of documents for all |
Eligibility Factors other than identity and |
citizenship/alien status are acceptable. |
|
Form |
Human Resources Administration |
Rev. 8/22/12 |
Family Independence Administration |
Eligibility Factor |
To prove this factor, provide ONE of the following: |
Unearned Income continued |
|
Other unearned income |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Resources |
• |
Statement from household |
||||
|
• Statement from nursing home |
||||||
(For Medical Assistance only, resource information is not |
|||||||
|
|
|
|
||||
requested from pregnant women, children under the age of 19 and |
|
|
|
|
|||
persons eligible for Family Health Plus.) |
|
|
|
|
|||
|
Bank Accounts: Checking, savings, retirement (IRA and |
• |
Current bank records |
||||
Keogh), credit union |
• |
Current credit card records |
|||||
|
|
|
• |
|
|
|
|
|
Stocks, bonds, certificates and mutual funds |
Stock/bond certificate |
|||||
|
|
|
• Statement from financial institution |
||||
|
|
|
• |
|
|
|
|
|
Life insurance |
Insurance policy |
|||||
|
|
|
• Statement from insurance company |
||||
|
|
|
• |
|
|
|
|
|
Burial trust or fund, burial plot or funeral agreement |
Bank records |
|||||
|
|
|
• |
Burial agreement |
|||
|
|
|
• |
Burial plot deed |
|||
|
|
|
• Statement from funeral director |
||||
|
Income tax refund or Earned Income Tax Credit (EITC) |
• |
Refund of EITC check |
||||
|
|
|
• Statement from tax office |
||||
|
Real estate other than residence |
• |
Deed |
||||
|
|
|
• Statement from real estate broker |
||||
|
|
|
• Broker’s appraisal/estimate of current value by broker |
||||
|
Motor vehicle |
• |
Registration (older models) |
||||
|
|
|
• |
Title of ownership |
|||
|
|
|
• Appraisal of current value by dealer |
||||
|
|
|
• |
Financing data |
|||
|
Lump sum payment |
• |
Statement from the source of payment |
||||
|
|
|
• |
Lump sum check |
|||
|
Other resources |
• |
Household statement of current value |
||||
|
|
|
• |
Sales slips |
|||
|
|
|
• |
Insurance appraisal |
|||
|
Shelter Expenses |
• Current rent receipt/lease/mortgage book/records |
|||||
|
• Property and school tax records |
||||||
|
|
|
|||||
You must prove how much it costs you to live where you do. (You |
• |
Landlord statement |
|||||
may need to provide separate documentation for each item of |
• |
Sewer and water bills |
|||||
shelter expense.) |
• |
Garbage/trash collection bills or receipts |
|||||
Medical Assistance does not require documentation of shelter |
• |
Homeowner’s insurance records |
|||||
expenses. |
|||||||
• Fuel |
|||||||
|
|
|
|||||
|
|
|
• |
Nonheating utility bills |
|||
|
|
|
• Telephone bills (or a statement from the household that the |
||||
|
|
|
|
expense is incurred) |
|||
|
Medical Expenses |
• Statement from provider of health insurance premiums |
|||||
|
• Copies of medical bills (paid and unpaid) |
||||||
For SNAP, for aged/disabled individuals only |
|||||||
• Medicare prescription drug card |
|||||||
|
|
|
|||||
|
|
|
|
|
|
|
|
Note: For SNAP, copies of documents are acceptable whenever proof of eligibility is presented. For Cash Assistance (CA) and Medical Assistance (MA), original documents are needed to verify identity and citizenship/alien status. Copies of documents for all Eligibility Factors other than identity and citizenship/alien status are acceptable.
Form |
Human Resources Administration |
Rev. 8/22/12 |
Family Independence Administration |
Eligibility Factor |
|
To prove this factor, provide ONE of the following: |
|
|
• |
Insurance policy/card |
|
Health Insurance |
• |
Statement from provider of coverage |
|
If you or anyone applying has health insurance coverage (even if |
• |
Medicare card |
|
• Separation or divorce agreement with |
|||
paid for by someone else), you must prove this. |
|||
|
coverage |
||
|
|
||
Disabled/Incapacitated/Pregnant |
• |
Statement from doctor, clinic or hospital verifying pregnancy, |
|
If you or anyone living with you is sick or pregnant, you must |
|
expected date of birth |
|
• Statement from medical professional |
|||
provide proof. |
|||
• |
|
||
(For MA only, resource information is not requested from pregnant |
Proof of SSA/SSI benefits for disability/blindness |
||
women, children and persons eligible for Family Health Plus). |
|
|
|
Unpaid Bills |
• Copy of each bill showing amount owed, period of |
||
• |
|
||
Rent, utility |
services and provider |
||
|
|
||
Referral |
• |
Statement from provider of treatment |
|
Drug/alcohol treatment program |
|
|
|
Employment service |
• Statement from employment service |
||
|
|
||
|
|
|
|
Other Expenses/Dependent Care Cost |
• |
Court order |
|
• Statement from day care center or other child care provider |
|||
|
|||
You must provide proof if you pay |
• |
Statement from aide or attendant |
|
care, recurring loans or for the services of a home health aide or |
• Canceled checks or receipts |
||
attendant. |
|||
|
|
||
School Attendance |
• School records (current report card) |
||
• Statement from school or higher education institution |
|||
You must prove who is in school. |
|||
|
|
||
|
|
|
|
Past Management |
• Letter from employer giving dates of employment, amount |
||
|
|||
(For Safety Net Assistance) |
|
earned and reason(s) for leaving |
|
|
If you were not supporting yourself from employment/earned |
||
Earned Income |
income, please bring verification of how you were able to support |
||
yourself in the past such as: |
|||
|
|||
|
• |
Bankbook/bank statement |
|
Other |
• Verification of expiration of benefits (workers’ compensation, |
||
|
disability, Social Security, UIB, etc.) |
||
|
|
||
(For cash assistance only) |
• |
Statement from person(s) who provided support |
|
|
|
||
Potential Benefits |
Statement from person(s) who provided support |
||
• If you or anyone in the household has applied for and been |
|||
|
|||
|
|
denied or has been accepted for benefits from any of the |
|
|
|
following sources, bring the award letter, check or other |
|
|
|
correspondence: Social Security, court payments, SSI, |
|
|
|
veteran’s benefits, workers’ compensation, union benefits, |
|
|
|
pension, military allotment, railroad retirement, NYS disability or |
|
|
|
other source |
|
Other |
|
|
|
|
|
|
|
Note: For SNAP, copies of documents are acceptable whenever proof of eligibility is presented. For Cash Assistance (CA) and Medical Assistance (MA), original documents are needed to verify identity and citizenship/alien status. Copies of documents for all Eligibility Factors other than identity and citizenship/alien status are acceptable.