Form WC 200A is a document that is used to report workers' compensation information in the state of Georgia. This form must be completed and filed by all employers who have at least one employee working in the state of Georgia. The information on this form will help the Georgia Workers' Compensation Division to ensure that employers are meeting their obligations under the law with respect to workers' compensation insurance. Employers who do not comply with the workers' compensation laws can face significant penalties. Completing and filing Form WC 200A is therefore very important for anyone doing business in Georgia.
| Question | Answer |
|---|---|
| Form Name | Form Wc 200A Georgia |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | workers compensation froms georgia, georgia 200a, wc change form, ga change workers compensation |
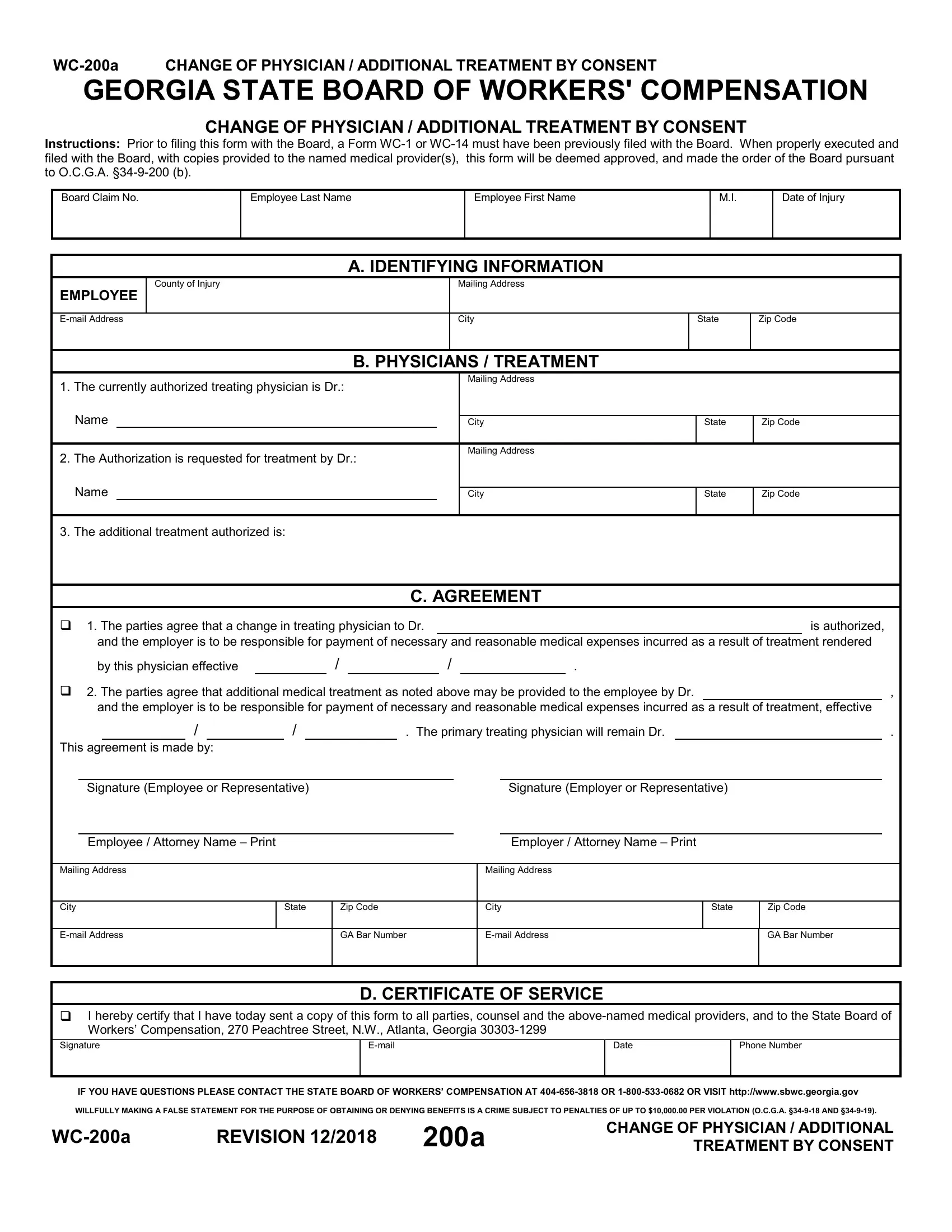
GEORGIA STATE BOARD OF WORKERS' COMPENSATION
CHANGE OF PHYSICIAN / ADDITIONAL TREATMENT BY CONSENT
Instructions: Prior to filing this form with the Board, a Form
Board Claim No.
Employee Last Name
Employee First Name
M.I.
Date of Injury
A. IDENTIFYING INFORMATION
EMPLOYEE
County of Injury
Mailing Address
City
State
Zip Code
B. PHYSICIANS / TREATMENT
1.The currently authorized treating physician is Dr.: Name
2.The Authorization is requested for treatment by Dr.:
Mailing Address
City
Mailing Address
State
Zip Code
Name
City
State
Zip Code
3. The additional treatment authorized is:
C. AGREEMENT
1. The parties agree that a change in treating physician to Dr. |
|
|
|
|
|
|
|
|
is authorized, |
||||||||||||||||
|
and the employer is to be responsible for payment of necessary and reasonable medical expenses incurred as a result of treatment rendered |
||||||||||||||||||||||||
|
by this physician effective |
|
|
|
/ |
|
|
/ |
|
|
. |
|
|
|
|
|
|||||||||
2. The parties agree that additional medical treatment as noted above may be provided to the employee by Dr. |
|
|
, |
||||||||||||||||||||||
|
and the employer is to be responsible for payment of necessary and reasonable medical expenses incurred as a result of treatment, effective |
||||||||||||||||||||||||
|
|
/ |
|
|
|
/ |
|
|
|
|
|
. The primary treating physician will remain Dr. |
|
|
|
. |
|||||||||
This agreement is made by: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
Signature (Employee or Representative) |
|
|
|
|
|
|
|
|
|
|
Signature (Employer or Representative) |
|
|
|
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
Employee / Attorney Name – Print |
|
|
|
|
|
|
|
|
|
|
|
|
Employer / Attorney Name – Print |
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||
Mailing Address |
|
|
|
|
|
|
|
|
|
|
|
Mailing Address |
|
|
|
|
|||||||||
|
|
|
|
|
|
|
|
|
|
||||||||||||||||
City |
|
State |
|
|
Zip Code |
|
City |
State |
Zip Code |
||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||
|
|
|
|
GA Bar Number |
|
|
GA Bar Number |
||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
D. CERTIFICATE OF SERVICE
I hereby certify that I have today sent a copy of this form to all parties, counsel and the
Signature |
Date |
Phone Number |
|
|
|
|
|
IF YOU HAVE QUESTIONS PLEASE CONTACT THE STATE BOARD OF WORKERS’ COMPENSATION AT
WILLFULLY MAKING A FALSE STATEMENT FOR THE PURPOSE OF OBTAINING OR DENYING BENEFITS IS A CRIME SUBJECT TO PENALTIES OF UP TO $10,000.00 PER VIOLATION (O.C.G.A.
REVISION 12/2018 |
200a |
CHANGE OF PHYSICIAN / ADDITIONAL |
|
TREATMENT BY CONSENT |